Department of Medical Oncology and Sarcoma Center, University Hospital Essen, Essen, Germany.
German Cancer Consortium (DKTK), Partner Site Essen, Germany.
J Clin Oncol. 2022 Dec 1;40(34):3918-3928. doi: 10.1200/JCO.22.00294. Epub 2022 Aug 10.
Sunitinib, a multitargeted tyrosine kinase inhibitor (TKI), is approved for advanced gastrointestinal stromal tumor (GIST) after imatinib failure. Ripretinib is a switch-control TKI approved for advanced GIST after prior treatment with three or more TKIs, including imatinib. We compared efficacy and safety of ripretinib versus sunitinib in patients with advanced GIST who were previously treated with imatinib (INTRIGUE, ClinicalTrials.gov identifier: NCT03673501).
Random assignment was 1:1 to once-daily ripretinib 150 mg or once-daily sunitinib 50 mg (4 weeks on/2 weeks off) and stratified by / mutation and imatinib intolerance. The primary end point was progression-free survival (PFS) by independent radiologic review using modified Response Evaluation Criteria in Solid Tumors version 1.1. Secondary end points included objective response rate by independent radiologic review, safety, and patient-reported outcome measures.
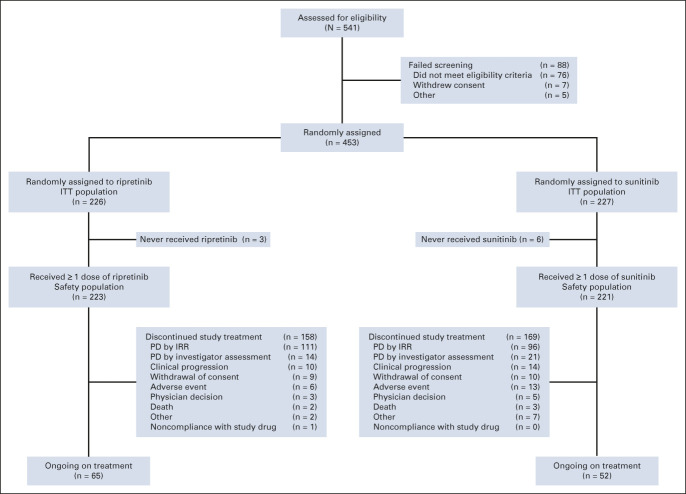
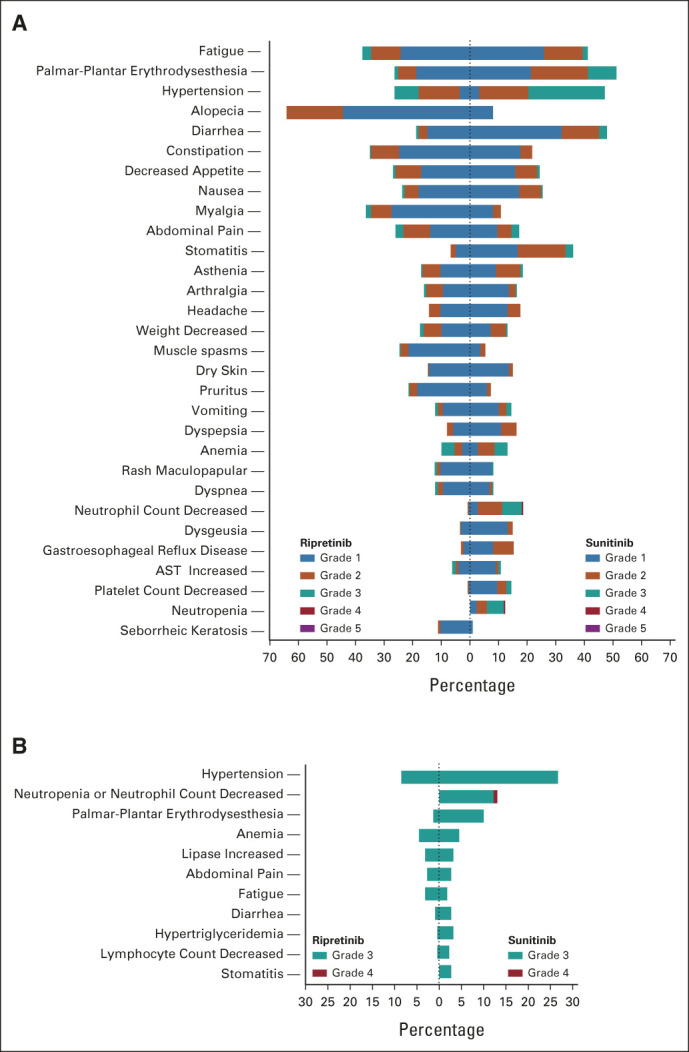
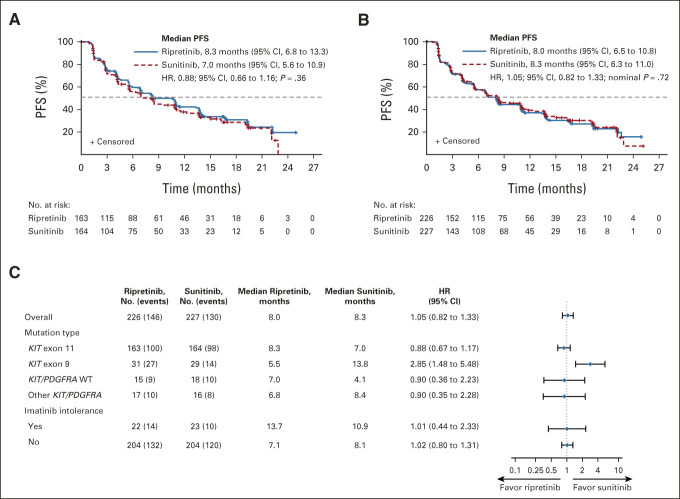
Overall, 453 patients were randomly assigned to ripretinib (intention-to-treat [ITT], n = 226; exon 11 ITT, n = 163) or sunitinib (ITT, n = 227; exon 11 ITT, n = 164). Median PFS for ripretinib and sunitinib ( exon 11 ITT) was 8.3 and 7.0 months, respectively (hazard ratio, 0.88; 95% CI, 0.66 to 1.16; = .36); median PFS (ITT) was 8.0 and 8.3 months, respectively (hazard ratio, 1.05; 95% CI, 0.82 to 1.33; nominal = .72). Neither was statistically significant. Objective response rate was higher for ripretinib versus sunitinib in the exon 11 ITT population (23.9% 14.6%, nominal = .03). Ripretinib was associated with a more favorable safety profile, fewer grade 3/4 treatment-emergent adverse events (41.3% 65.6%, nominal < .0001), and better scores on patient-reported outcome measures of tolerability.
Ripretinib was not superior to sunitinib in terms of PFS. However, meaningful clinical activity, fewer grade 3/4 treatment-emergent adverse events, and improved tolerability were observed with ripretinib.
舒尼替尼是一种多靶点酪氨酸激酶抑制剂(TKI),在伊马替尼治疗失败后被批准用于晚期胃肠道间质瘤(GIST)。瑞普替尼是一种开关控制 TKI,在先前接受过三种或更多种 TKI(包括伊马替尼)治疗的晚期 GIST 患者中被批准使用。我们比较了瑞普替尼与舒尼替尼在先前接受过伊马替尼治疗的晚期 GIST 患者中的疗效和安全性(INTRIGUE,ClinicalTrials.gov 标识符:NCT03673501)。
随机分配比例为 1:1,每日一次瑞普替尼 150mg 或每日一次舒尼替尼 50mg(4 周用药/2 周停药),并根据 / 突变和伊马替尼不耐受进行分层。主要终点是独立影像学评估使用改良的实体瘤反应评估标准 1.1 评估的无进展生存期(PFS)。次要终点包括独立影像学评估的客观缓解率、安全性和患者报告的结局测量。
共有 453 名患者被随机分配至瑞普替尼(意向治疗[ITT],n=226; exon 11 ITT,n=163)或舒尼替尼(ITT,n=227;exon 11 ITT,n=164)。瑞普替尼和舒尼替尼(exon 11 ITT)的中位 PFS 分别为 8.3 个月和 7.0 个月(风险比,0.88;95%CI,0.66 至 1.16; =.36);中位 PFS(ITT)分别为 8.0 个月和 8.3 个月(风险比,1.05;95%CI,0.82 至 1.33;名义 =.72)。两者均无统计学意义。瑞普替尼在 exon 11 ITT 人群中的客观缓解率高于舒尼替尼(23.9% 14.6%,名义 =.03)。瑞普替尼与更有利的安全性相关,治疗相关不良事件 3/4 级发生率较低(41.3% 65.6%,名义 <.0001),且患者报告的耐受性结局测量得分更好。
在 PFS 方面,瑞普替尼并不优于舒尼替尼。然而,瑞普替尼观察到了更有意义的临床活性、更低的 3/4 级治疗相关不良事件和更好的耐受性。