Department of Clinical Pathology and Centre for Cancer Research, University of Melbourne, Melbourne, VIC, Australia.
Department of Pathology, Peter MacCallum Cancer Centre, Melbourne, VIC, Australia.
J Pathol. 2023 Jan;259(1):81-92. doi: 10.1002/path.6022. Epub 2022 Nov 30.
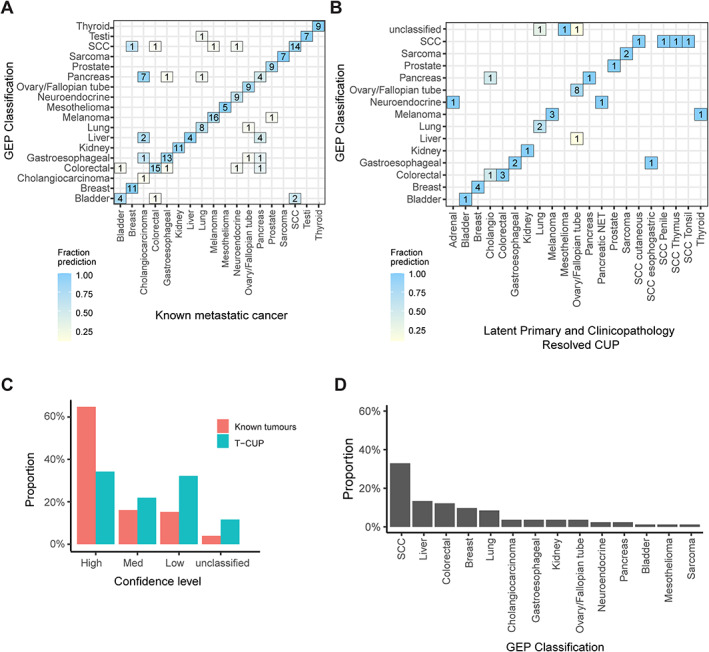
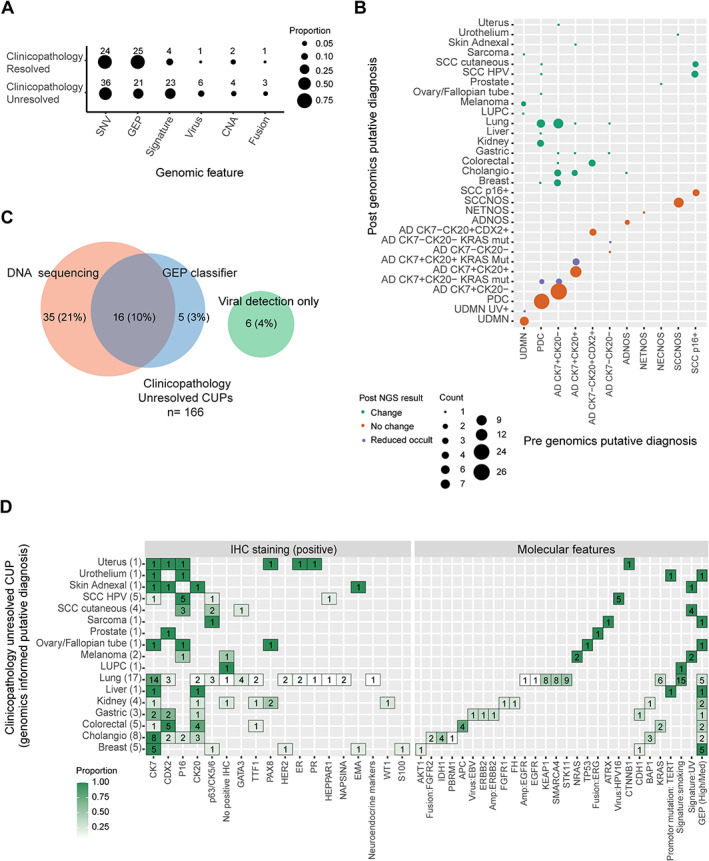
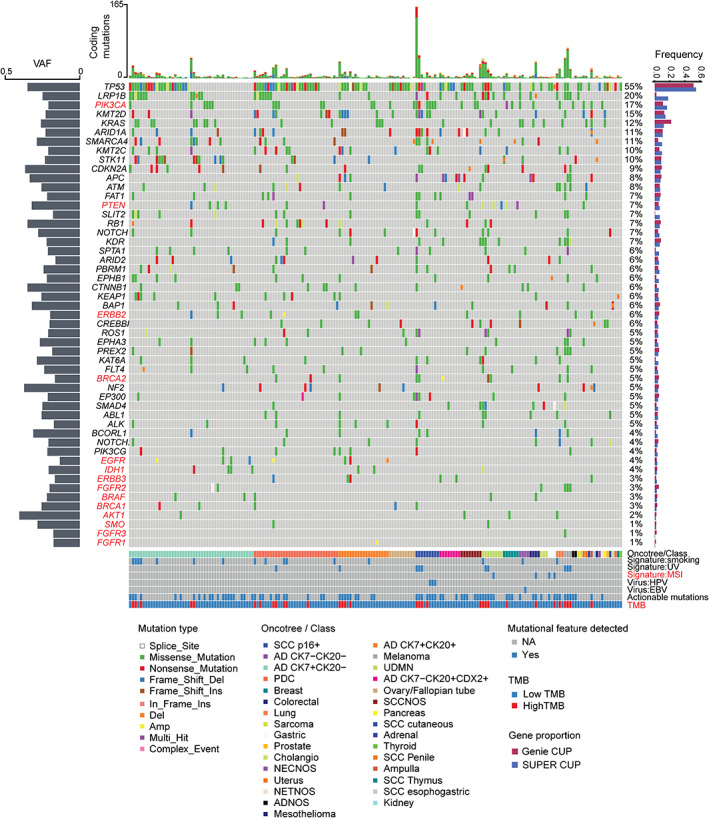
Cancer of unknown primary (CUP) is a syndrome defined by clinical absence of a primary cancer after standardised investigations. Gene expression profiling (GEP) and DNA sequencing have been used to predict primary tissue of origin (TOO) in CUP and find molecularly guided treatments; however, a detailed comparison of the diagnostic yield from these two tests has not been described. Here, we compared the diagnostic utility of RNA and DNA tests in 215 CUP patients (82% received both tests) in a prospective Australian study. Based on retrospective assessment of clinicopathological data, 77% (166/215) of CUPs had insufficient evidence to support TOO diagnosis (clinicopathology unresolved). The remainder had either a latent primary diagnosis (10%) or clinicopathological evidence to support a likely TOO diagnosis (13%) (clinicopathology resolved). We applied a microarray (CUPGuide) or custom NanoString 18-class GEP test to 191 CUPs with an accuracy of 91.5% in known metastatic cancers for high-medium confidence predictions. Classification performance was similar in clinicopathology-resolved CUPs - 80% had high-medium predictions and 94% were concordant with pathology. Notably, only 56% of the clinicopathology-unresolved CUPs had high-medium confidence GEP predictions. Diagnostic DNA features were interrogated in 201 CUP tumours guided by the cancer type specificity of mutations observed across 22 cancer types from the AACR Project GENIE database (77,058 tumours) as well as mutational signatures (e.g. smoking). Among the clinicopathology-unresolved CUPs, mutations and mutational signatures provided additional diagnostic evidence in 31% of cases. GEP classification was useful in only 13% of cases and oncoviral detection in 4%. Among CUPs where genomics informed TOO, lung and biliary cancers were the most frequently identified types, while kidney tumours were another identifiable subset. In conclusion, DNA and RNA profiling supported an unconfirmed TOO diagnosis in one-third of CUPs otherwise unresolved by clinicopathology assessment alone. DNA mutation profiling was the more diagnostically informative assay. © 2022 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
原发灶不明癌(CUP)是一种综合征,其定义为经过标准检查后临床仍未发现原发性肿瘤。基因表达谱(GEP)和 DNA 测序已被用于预测 CUP 的原发组织来源(TOO)并寻找分子指导的治疗方法;然而,尚未详细比较这两种检测方法的诊断效果。在此,我们在一项澳大利亚前瞻性研究中比较了 215 例 CUP 患者(82%同时接受了这两种检测)的 RNA 和 DNA 检测的诊断效用。基于对临床病理数据的回顾性评估,77%(166/215)的 CUP 证据不足,无法支持 TOO 诊断(临床病理未解决)。其余的 CUP 要么存在潜在的原发性诊断(10%),要么存在支持可能的 TOO 诊断的临床病理证据(13%)(临床病理已解决)。我们对 191 例 CUP 应用了微阵列(CUPGuide)或定制的 NanoString 18 类 GEP 检测,在已知转移性癌症中的准确率为 91.5%,可进行高-中置信度预测。分类性能在临床病理已解决的 CUP 中相似 - 80%有高-中置信度预测,94%与病理学一致。值得注意的是,只有 56%的临床病理未解决的 CUP 具有高-中置信度的 GEP 预测。在由 AACR Project GENIE 数据库(77058 个肿瘤)中观察到的突变的癌症类型特异性以及突变特征(例如吸烟)指导下,对 201 个 CUP 肿瘤进行了 DNA 特征检测。在临床病理未解决的 CUP 中,突变和突变特征在 31%的病例中提供了额外的诊断证据。GEP 分类在 13%的病例中有用,oncoviral 检测在 4%的病例中有用。在基因组学提示 TOO 的 CUP 中,肺癌和胆管癌是最常确定的类型,而肾脏肿瘤是另一个可识别的亚组。总之,DNA 和 RNA 谱分析支持三分之一的 CUP 除了临床病理评估外,无法确定 TOO 诊断。DNA 突变谱分析是更具诊断意义的检测方法。