Department of Medicine, Division of Infectious Diseases, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Department of Medicine, David Geffen School of Medicine, University of California, Los Angeles, CA, USA.
Nat Microbiol. 2022 Nov;7(11):1906-1917. doi: 10.1038/s41564-022-01254-1. Epub 2022 Oct 26.
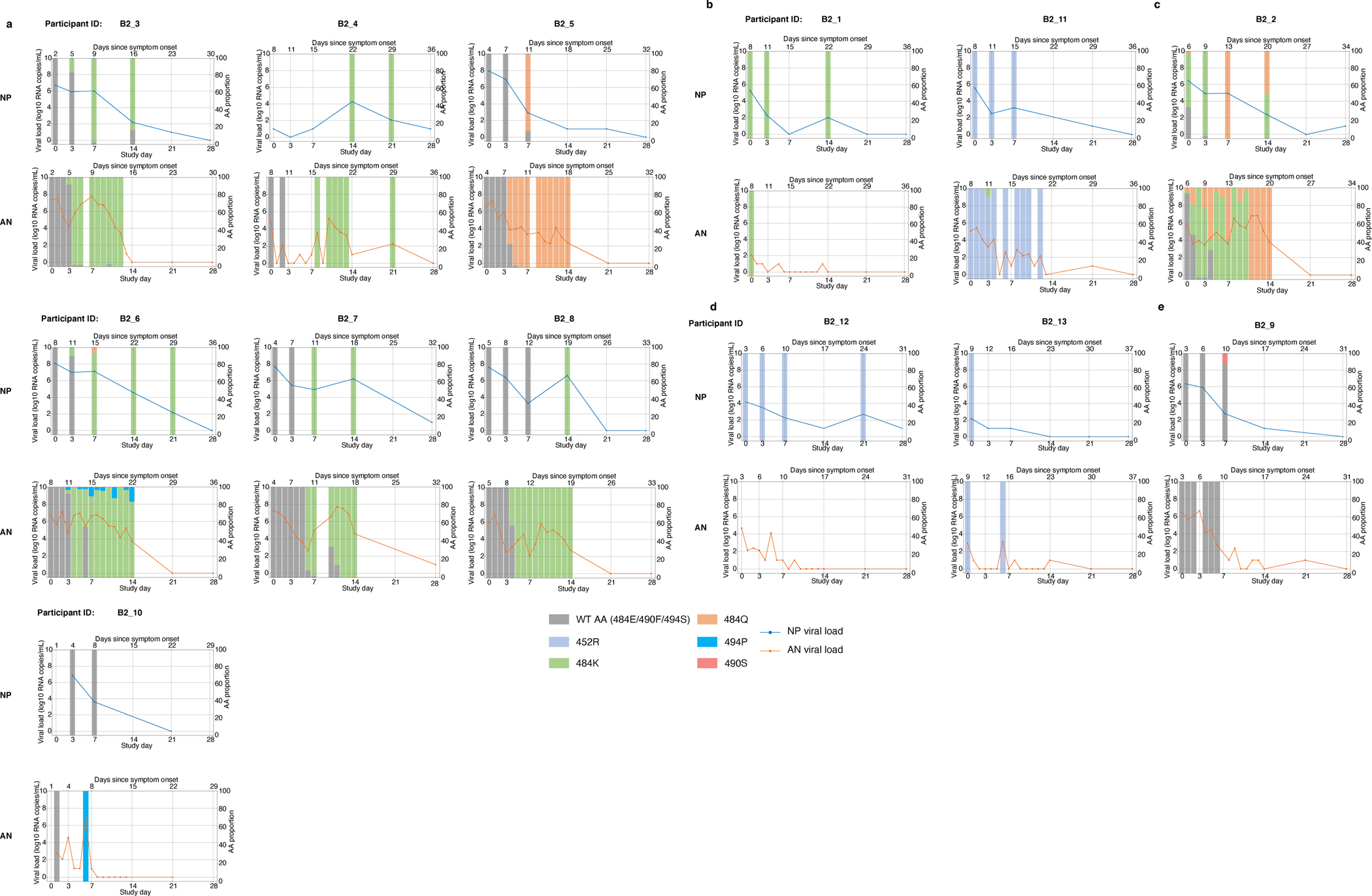
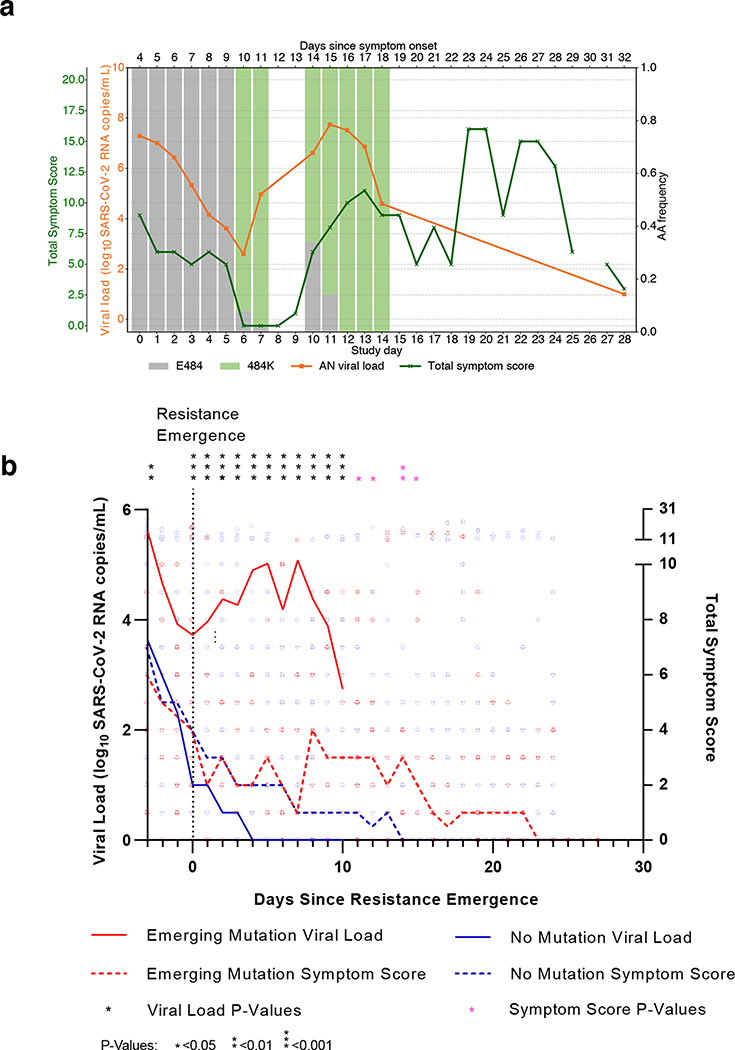
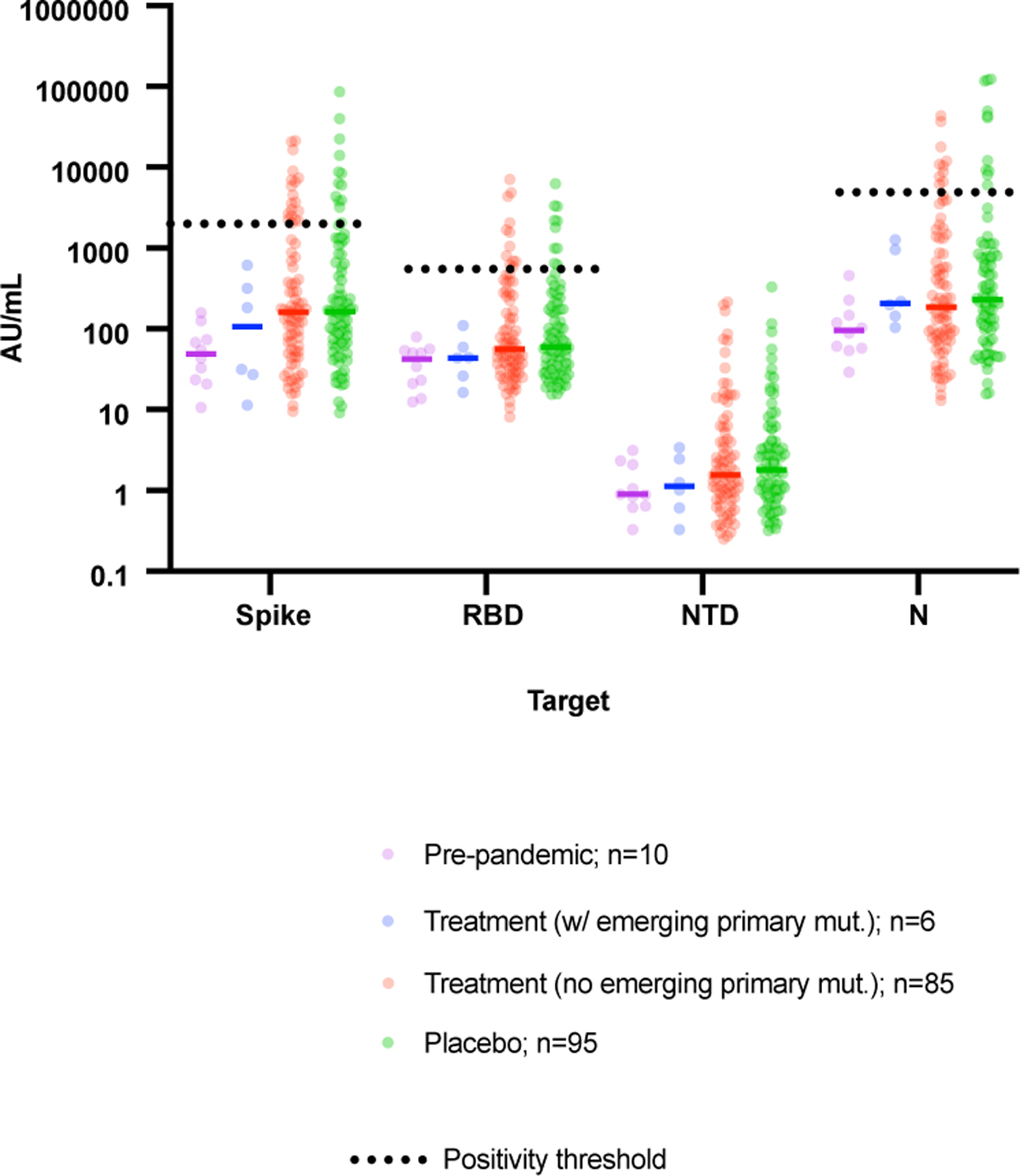
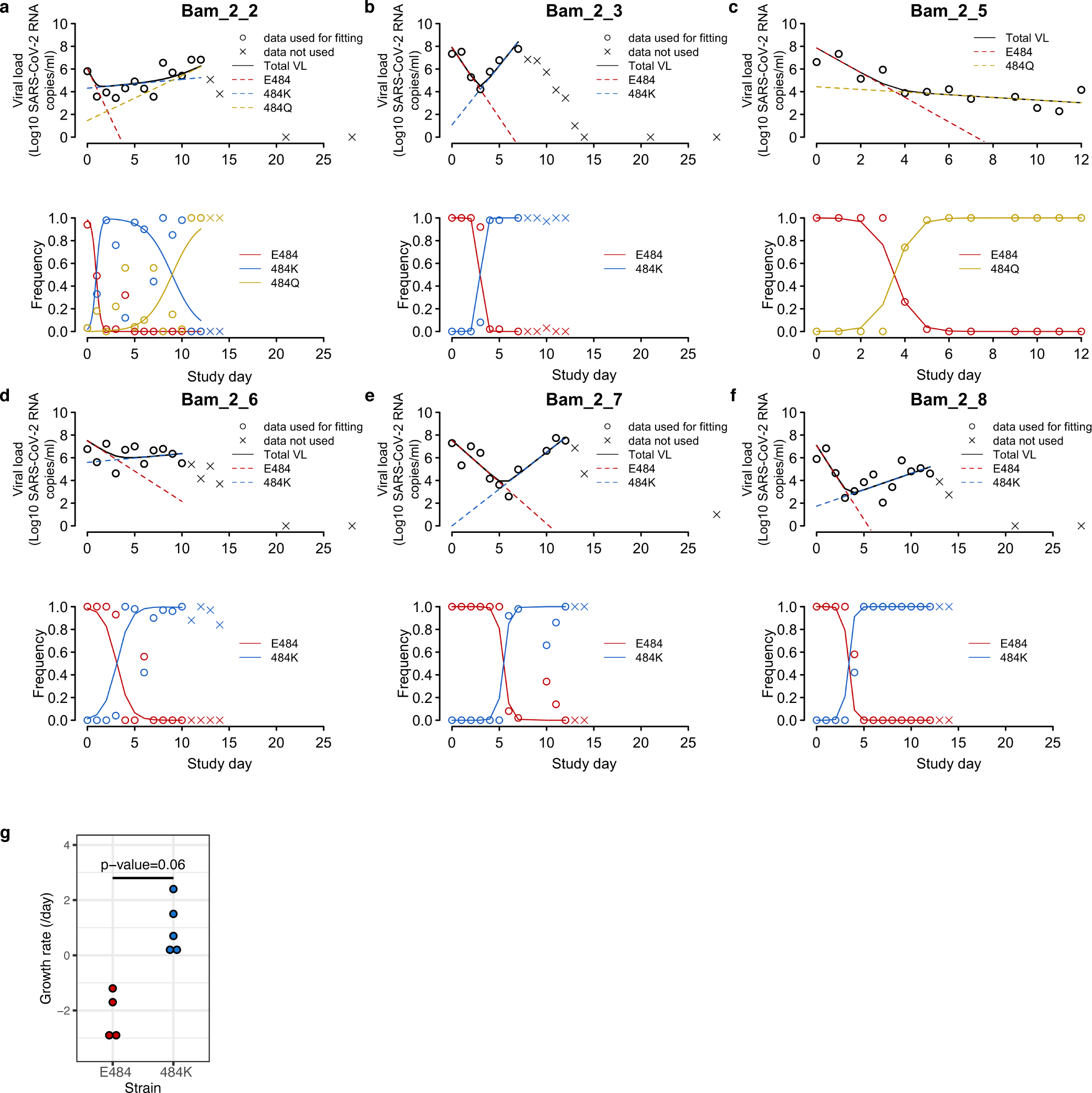
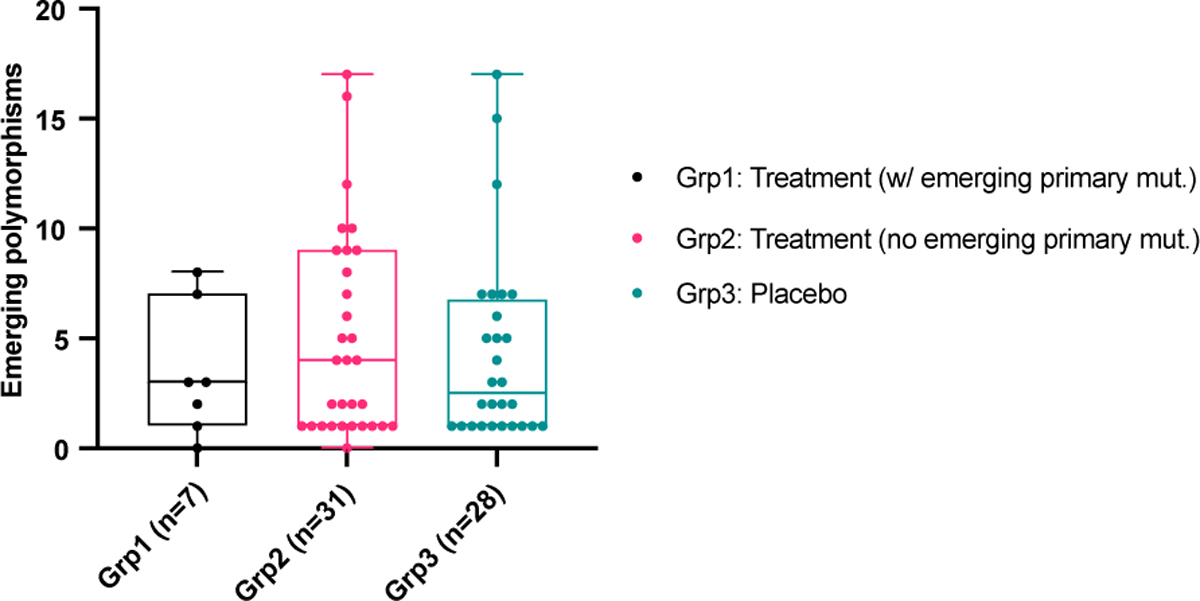
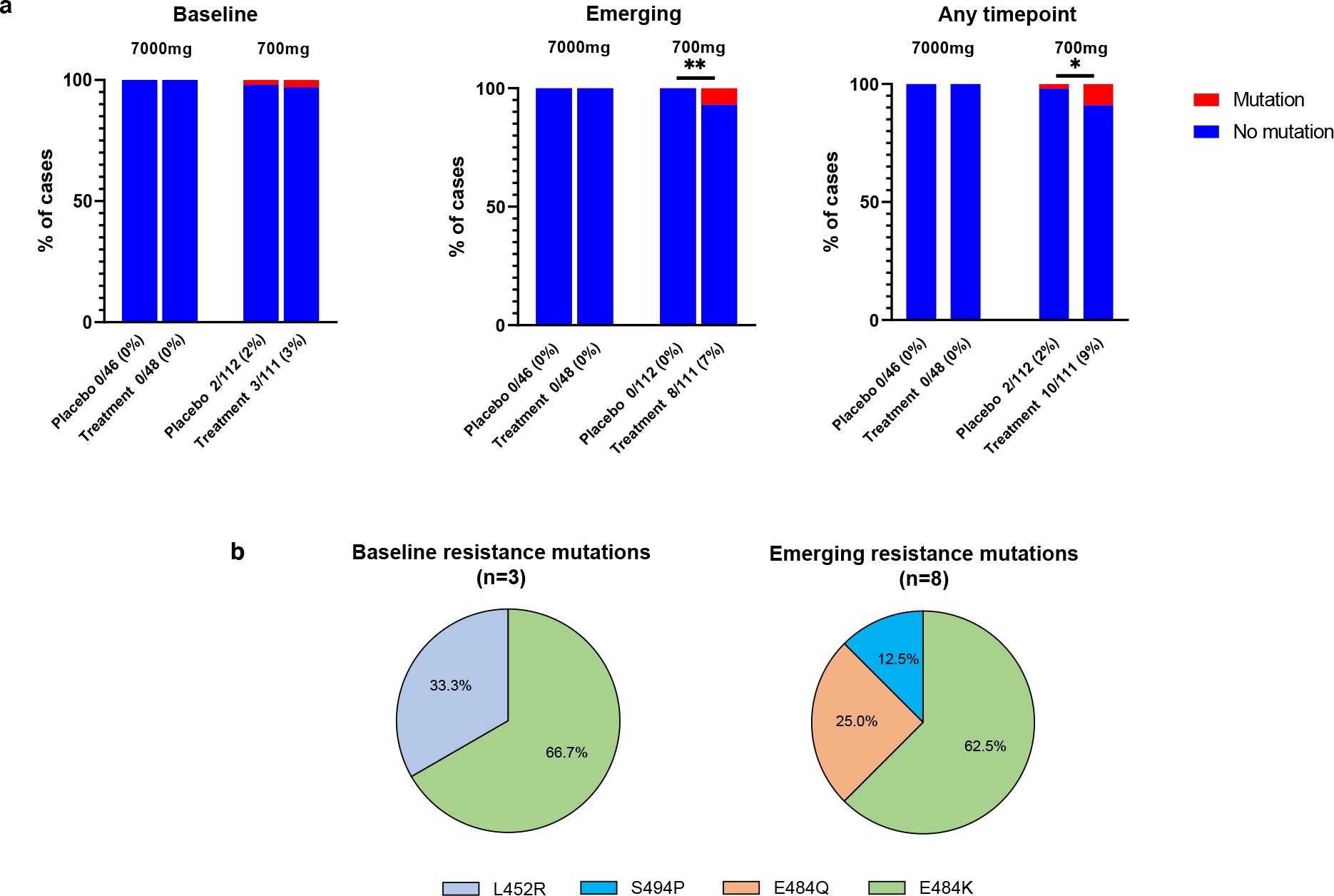
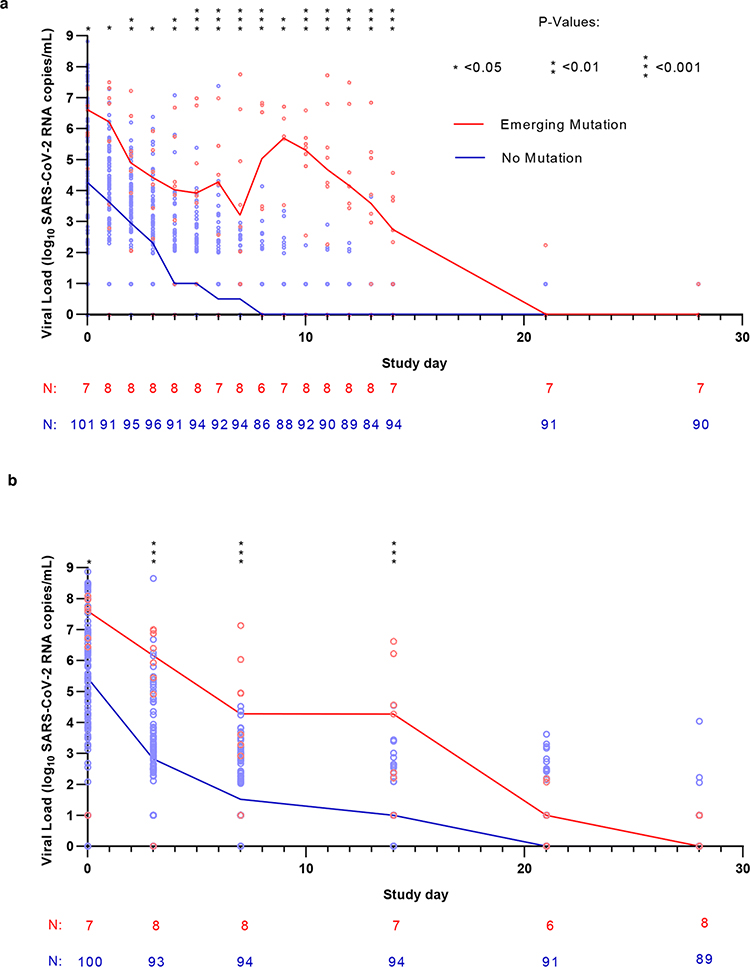
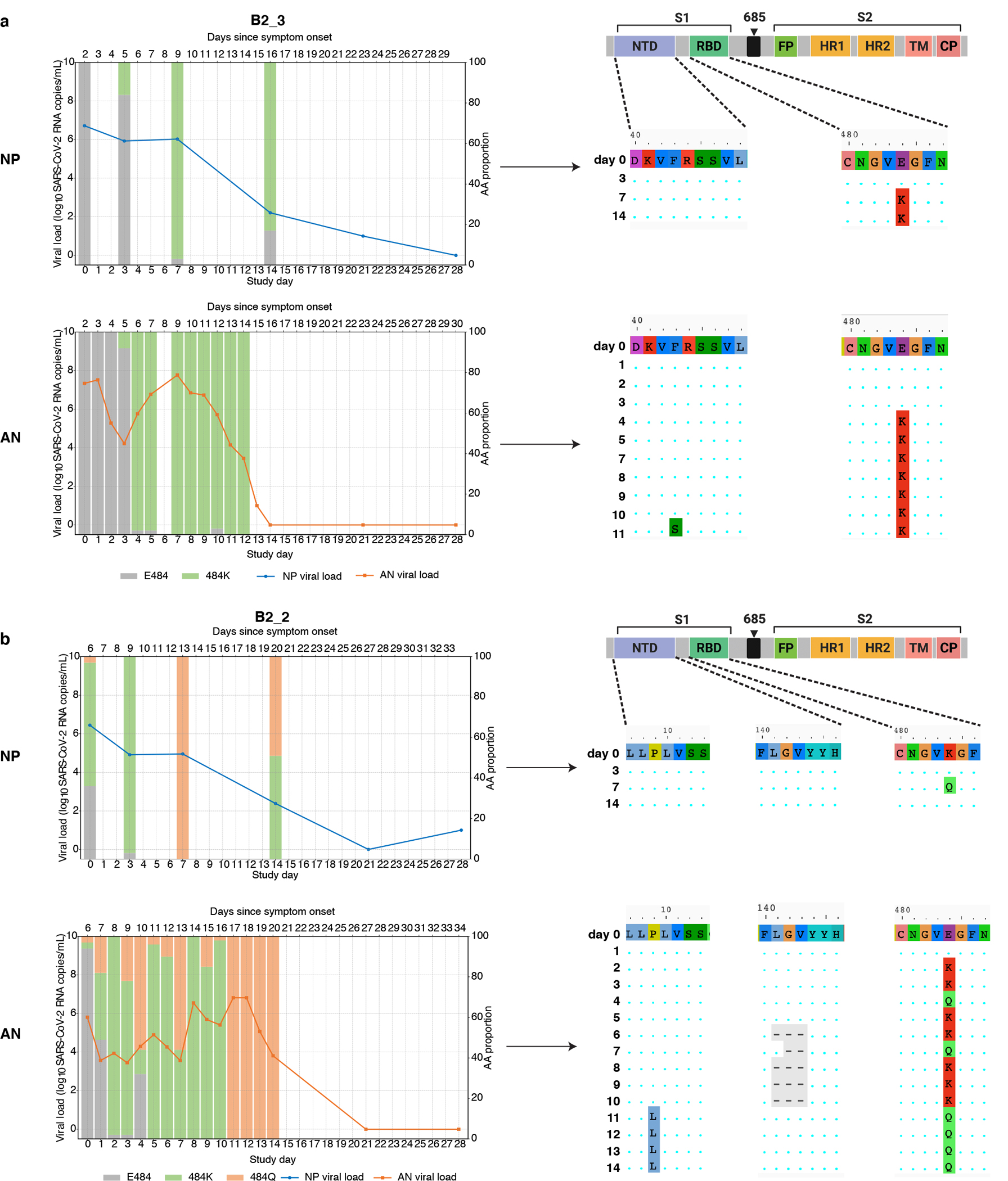
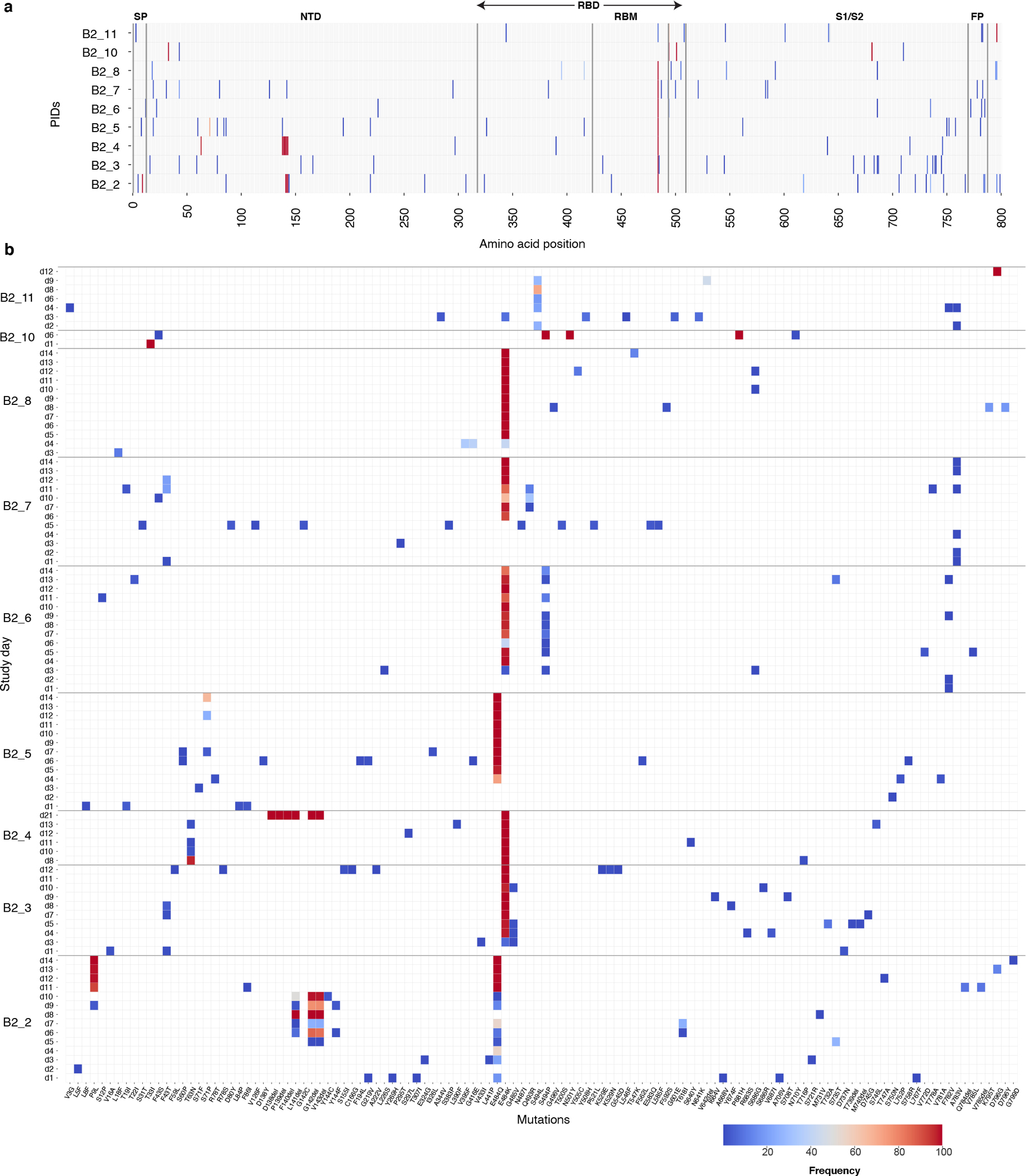
SARS-CoV-2 mutations that cause resistance to monoclonal antibody (mAb) therapy have been reported. However, it remains unclear whether in vivo emergence of SARS-CoV-2 resistance mutations alters viral replication dynamics or therapeutic efficacy in the immune-competent population. As part of the ACTIV-2/A5401 randomized clinical trial (NCT04518410), non-hospitalized participants with symptomatic SARS-CoV-2 infection were given bamlanivimab (700 mg or 7,000 mg) or placebo treatment. Here¸ we report that treatment-emergent resistance mutations [detected through targeted Spike (S) gene next-generation sequencing] were significantly more likely to be detected after bamlanivimab 700 mg treatment compared with the placebo group (7% of 111 vs 0% of 112 participants, P = 0.003). No treatment-emergent resistance mutations among the 48 participants who received 7,000 mg bamlanivimab were recorded. Participants in which emerging mAb resistant virus mutations were identified showed significantly higher pretreatment nasopharyngeal and anterior nasal viral loads. Daily respiratory tract viral sampling through study day 14 showed the dynamic nature of in vivo SARS-CoV-2 infection and indicated a rapid and sustained viral rebound after the emergence of resistance mutations. Participants with emerging bamlanivimab resistance often accumulated additional polymorphisms found in current variants of concern/interest that are associated with immune escape. These results highlight the potential for rapid emergence of resistance during mAb monotherapy treatment that results in prolonged high-level respiratory tract viral loads. Assessment of viral resistance should be prioritized during the development and clinical implementation of antiviral treatments for COVID-19.
SARS-CoV-2 突变可导致对单克隆抗体 (mAb) 治疗产生耐药性,这已得到报道。然而,尚不清楚体内 SARS-CoV-2 耐药突变的出现是否会改变免疫功能正常人群中的病毒复制动力学或治疗效果。作为 ACTIV-2/A5401 随机临床试验 (NCT04518410) 的一部分,对有症状的 SARS-CoV-2 感染的非住院患者给予 bamlanivimab (700mg 或 7000mg) 或安慰剂治疗。在这里,我们报告说,通过靶向 Spike (S) 基因下一代测序检测到的治疗中出现的耐药突变,在接受 bamlanivimab 700mg 治疗的患者中明显比安慰剂组更有可能被检测到 (111 名患者中有 7%,112 名患者中有 0%,P=0.003)。接受 7000mg bamlanivimab 治疗的 48 名患者中没有记录到治疗中出现的耐药突变。出现 mAb 耐药病毒突变的参与者的鼻咽和前鼻病毒载量明显更高。通过研究第 14 天的每日呼吸道病毒采样显示了体内 SARS-CoV-2 感染的动态特性,并表明在耐药突变出现后,病毒迅速且持续反弹。出现 bamlanivimab 耐药的参与者经常积累了当前关注/感兴趣的变异株中发现的额外的与免疫逃避相关的多态性。这些结果强调了在 mAb 单药治疗期间耐药性迅速出现的可能性,导致呼吸道病毒载量长时间处于高水平。在开发和临床实施 COVID-19 的抗病毒治疗时,应优先评估病毒耐药性。