Amioka Kei, Kawaoka Tomokazu, Kinami Takahiro, Yamasaki Shintaro, Kosaka Masanari, Johira Yusuke, Yano Shigeki, Naruto Kensuke, Ando Yuwa, Fujii Yasutoshi, Uchikawa Shinsuke, Ono Atsushi, Yamauchi Masami, Imamura Michio, Kosaka Yumi, Ohya Kazuki, Mori Nami, Takaki Shintaro, Tsuji Keiji, Masaki Keiichi, Honda Yoji, Kouno Hirotaka, Kohno Hioshi, Morio Kei, Moriya Takashi, Naeshiro Noriaki, Nonaka Michihiro, Aisaka Yasuyuki, Azakami Takahiro, Hiramatsu Akira, Aikata Hiroshi, Oka Shiro
Department of Gastroenterology and Metabolism, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima 734-8551, Japan.
Department of Gastroenterology, Hiroshima Red Cross Hospital & Atomic-Bomb Survivors Hospital, Hiroshima 730-8619, Japan.
Cancers (Basel). 2022 Oct 16;14(20):5066. doi: 10.3390/cancers14205066.
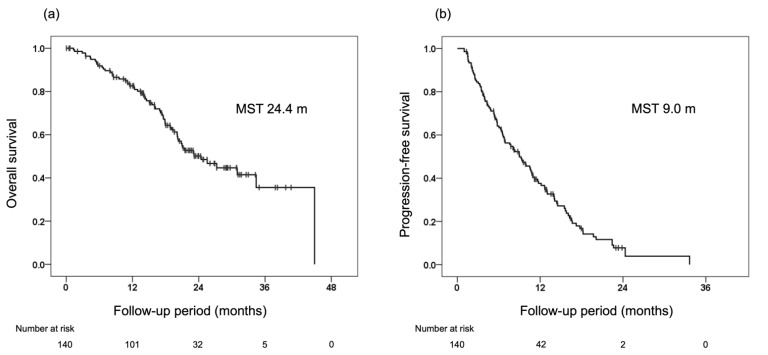
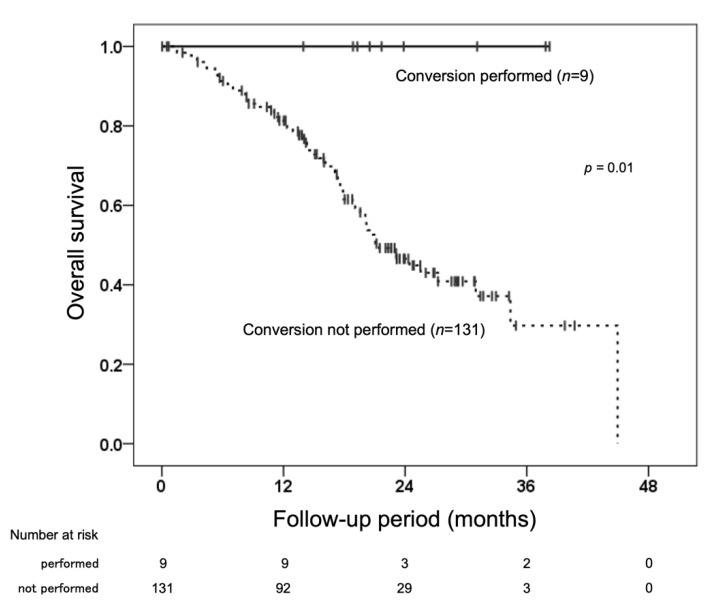
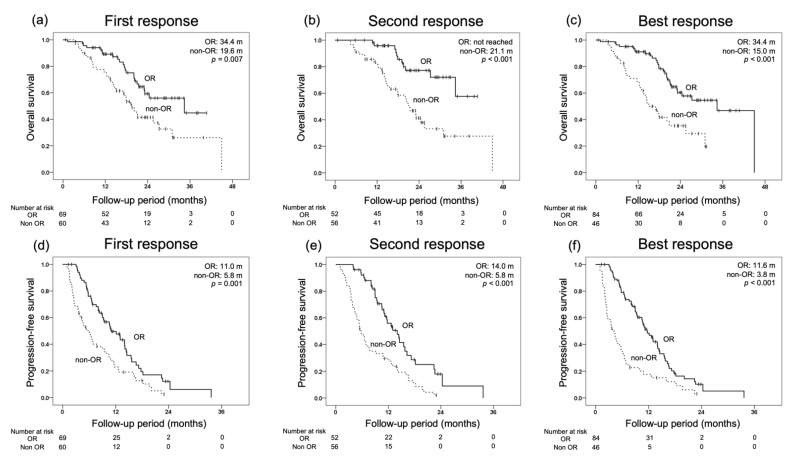
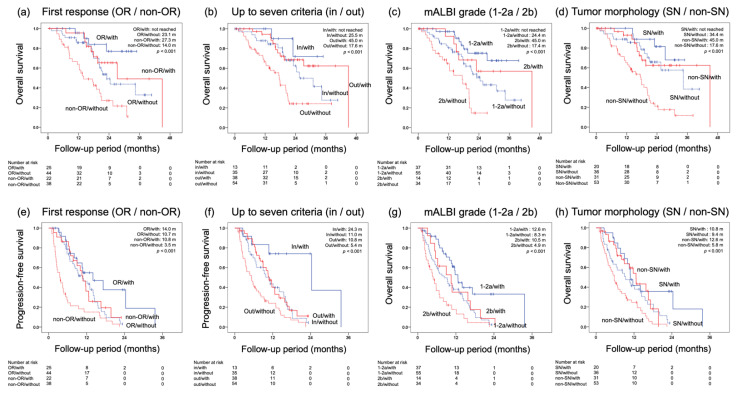
Transarterial chemoembolization (TACE) has been the standard treatment for intermediate-stage, unresectable hepatocellular carcinoma (u-HCC). However, with recent advances in systemic therapy and the emergence of the concept of TACE-refractory or -unsuitable, the effectiveness of systemic therapy, as well as TACE, has been demonstrated for patients judged to be TACE-refractory or -unsuitable. In this study, the efficacy of lenvatinib and its combination with TACE after lenvatinib was investigated in 140 patients with intermediate-stage u-HCC treated with lenvatinib mainly because of being judged to be TACE-refractory or -unsuitable. Median overall survival (OS) and progression-free survival (PFS) were 24.4 and 9.0 months, respectively, indicating a good response rate. In multivariate analysis, modified albumin-bilirubin (mALBI) grade and up to seven criteria were identified as independent factors for OS, and mALBI grade and tumor morphology were identified as independent factors for PFS. While 95% of all patients were TACE-refractory or -unsuitable, the further prognosis was prolonged by the combination with TACE after lenvatinib initiation. These findings suggest that systemic therapy should be considered for intermediate-stage u-HCC, even in patients judged to be TACE-refractory or -unsuitable. The use of TACE after the start of systemic therapy may further improve prognosis.
经动脉化疗栓塞术(TACE)一直是中期不可切除肝细胞癌(u-HCC)的标准治疗方法。然而,随着全身治疗的最新进展以及TACE难治或不适用概念的出现,对于被判定为TACE难治或不适用的患者,全身治疗以及TACE的有效性已得到证实。在本研究中,对140例主要因被判定为TACE难治或不适用而接受乐伐替尼治疗的中期u-HCC患者,研究了乐伐替尼及其与乐伐替尼后TACE联合治疗的疗效。中位总生存期(OS)和无进展生存期(PFS)分别为24.4个月和9.0个月,表明缓解率良好。在多变量分析中,改良白蛋白-胆红素(mALBI)分级和多达七个标准被确定为OS的独立因素,mALBI分级和肿瘤形态被确定为PFS的独立因素。虽然所有患者中有95%为TACE难治或不适用,但在开始使用乐伐替尼后联合TACE可延长进一步的预后。这些发现表明,即使是被判定为TACE难治或不适用的中期u-HCC患者,也应考虑全身治疗。在全身治疗开始后使用TACE可能会进一步改善预后。