Tettero Jesse M, Al-Badri Waleed K W, Ngai Lok Lam, Bachas Costa, Breems Dimitri A, van Elssen Catharina H M J, Fischer Thomas, Gjertsen Bjorn T, van Gorkom Gwendolyn N Y, Gradowska Patrycja, Greuter Marjolein J E, Griskevicius Laimonas, Juliusson Gunnar, Maertens Johan, Manz Markus G, Pabst Thomas, Passweg Jakob, Porkka Kimmo, Löwenberg Bob, Ossenkoppele Gert J, Janssen Jeroen J W M, Cloos Jacqueline
Department of Hematology, Amsterdam Univerisity Medical Centers location Vrije Universiteit Amsterdam, Amsterdam, Netherlands.
Cancer Center Amsterdam, Imaging and Biomarkers, Amsterdam, Netherlands.
Front Oncol. 2022 Oct 10;12:999822. doi: 10.3389/fonc.2022.999822. eCollection 2022.
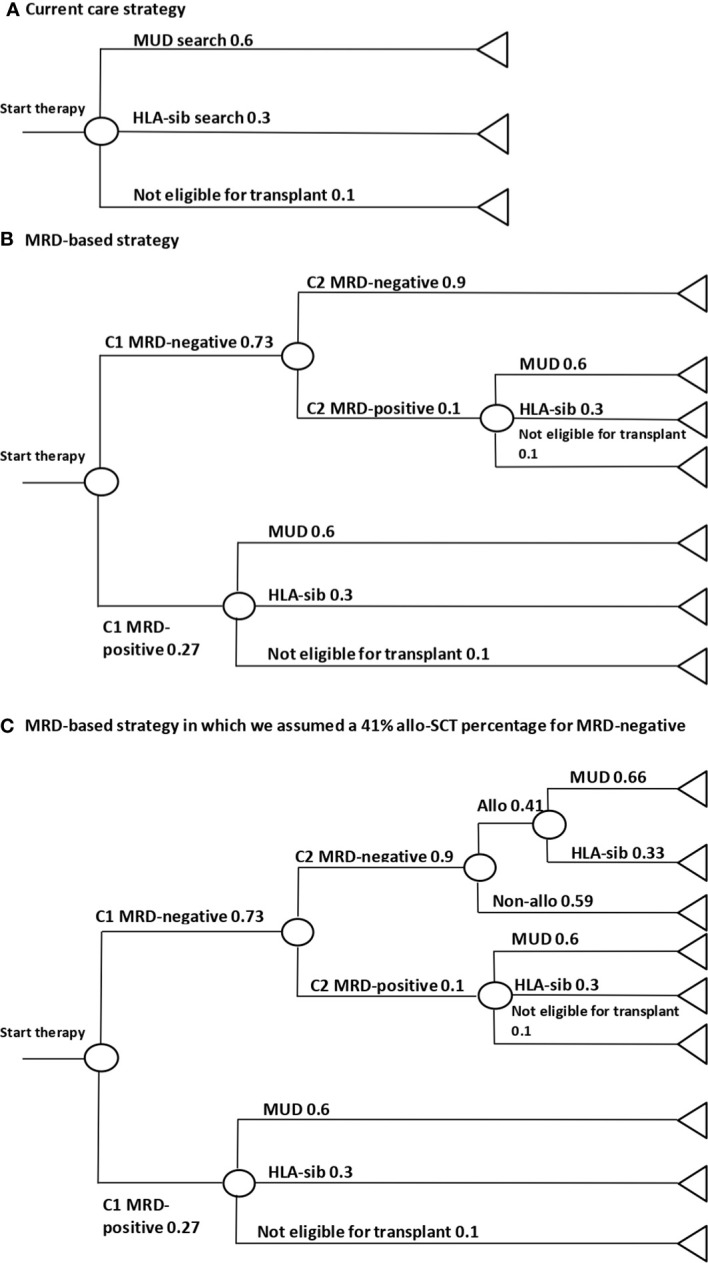
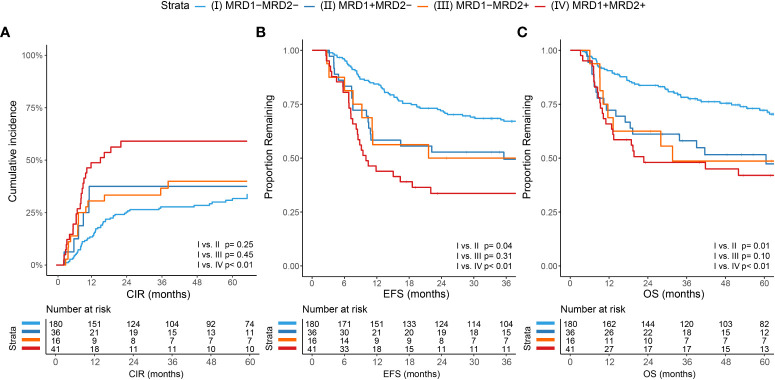
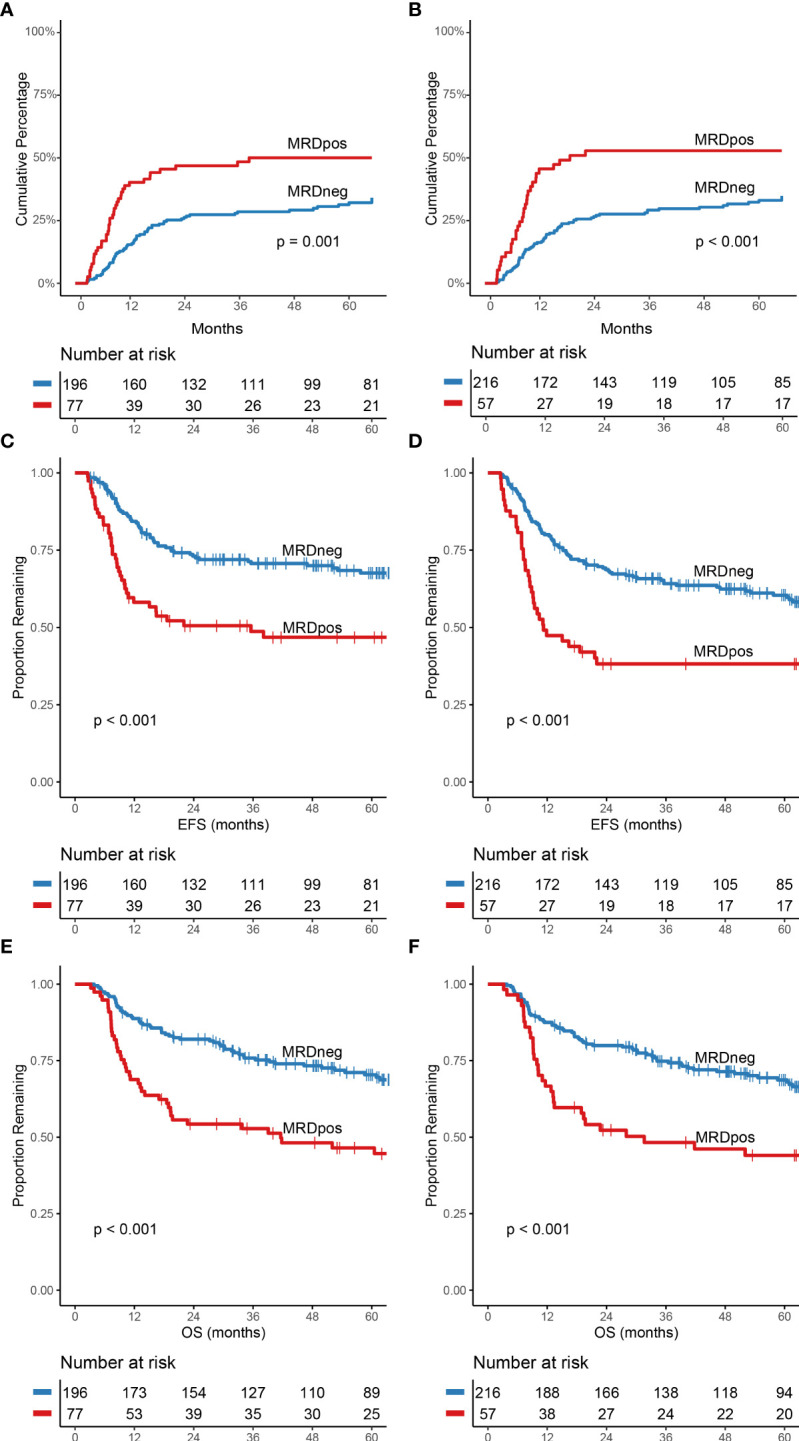
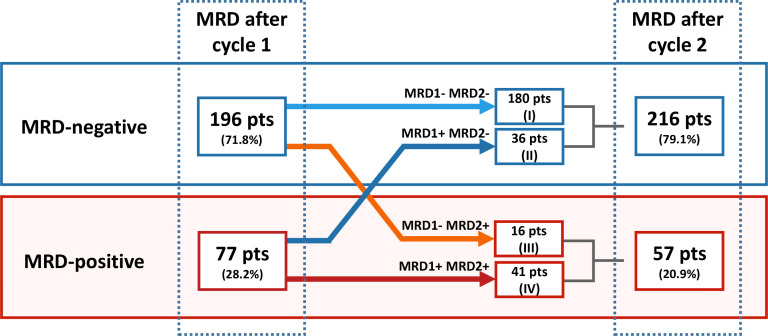
Measurable residual disease (MRD) measured using multiparameter flow-cytometry (MFC) has proven to be an important prognostic biomarker in acute myeloid leukemia (AML). In addition, MRD is increasingly used to guide consolidation treatment towards a non-allogenic stem cell transplantation treatment for MRD-negative patients in the ELN-2017 intermediate risk group. Currently, measurement of MFC-MRD in bone marrow is used for clinical decision making after 2 cycles of induction chemotherapy. However, measurement after 1 cycle has also been shown to have prognostic value, so the optimal time point remains a question of debate. We assessed the independent prognostic value of MRD results at either time point and concordance between these for 273 AML patients treated within and according to the HOVON-SAKK 92, 102, 103 and 132 trials. Cumulative incidence of relapse, event free survival and overall survival were significantly better for MRD-negative (<0.1%) patients compared to MRD-positive patients after cycle 1 and cycle 2 ( 0.002, for all comparisons). A total of 196 patients (71.8%) were MRD-negative after cycle 1, of which the vast majority remained negative after cycle 2 (180 patients; 91.8%). In contrast, of the 77 MRD-positive patients after cycle 1, only 41 patients (53.2%) remained positive. A cost reduction of -€571,751 per 100 patients could be achieved by initiating the donor search based on the MRD-result after cycle 1. This equals to a 50.7% cost reduction compared to the current care strategy in which the donor search is initiated for all patients. These results show that MRD after cycle 1 has prognostic value and is highly concordant with MRD status after cycle 2. When MRD-MFC is used to guide consolidation treatment (allo vs non-allo) in intermediate risk patients, allogeneic donor search may be postponed or omitted after cycle 1. Since the majority of MRD-negative patients remain negative after cycle 2, this could safely reduce the number of allogeneic donor searches and reduce costs.
使用多参数流式细胞术(MFC)检测的可测量残留病(MRD)已被证明是急性髓系白血病(AML)中一种重要的预后生物标志物。此外,MRD越来越多地用于指导ELN - 2017中危组MRD阴性患者进行非异基因干细胞移植治疗的巩固治疗。目前,在诱导化疗2个周期后,骨髓中MFC - MRD的检测用于临床决策。然而,1个周期后的检测也显示具有预后价值,因此最佳时间点仍是一个有争议的问题。我们评估了HOVON - SAKK 92、102、103和132试验中273例接受治疗的AML患者在这两个时间点MRD结果的独立预后价值以及它们之间的一致性。与第1周期和第2周期后MRD阳性患者相比,MRD阴性(<0.1%)患者的累积复发率、无事件生存率和总生存率显著更好(所有比较P < 0.002)。共有196例患者(71.8%)在第1周期后MRD阴性,其中绝大多数在第2周期后仍为阴性(180例患者;91.8%)。相比之下,在第1周期后77例MRD阳性患者中,只有41例患者(53.2%)仍为阳性。根据第1周期后的MRD结果启动供体搜索,每100例患者可节省成本571,751欧元。与目前对所有患者启动供体搜索的护理策略相比,这相当于成本降低了50.7%。这些结果表明,第1周期后的MRD具有预后价值,并且与第2周期后的MRD状态高度一致。当MRD - MFC用于指导中危患者的巩固治疗(异基因移植与非异基因移植)时,第1周期后可推迟或省略异基因供体搜索。由于大多数MRD阴性患者在第2周期后仍为阴性,这可以安全地减少异基因供体搜索的数量并降低成本。