Department of Hematology, Amsterdam University Medical Center (UMC), Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Imaging and Biomarkers, Cancer Center Amsterdam, Amsterdam, The Netherlands.
Blood Adv. 2023 Jan 24;7(2):214-223. doi: 10.1182/bloodadvances.2022008629.
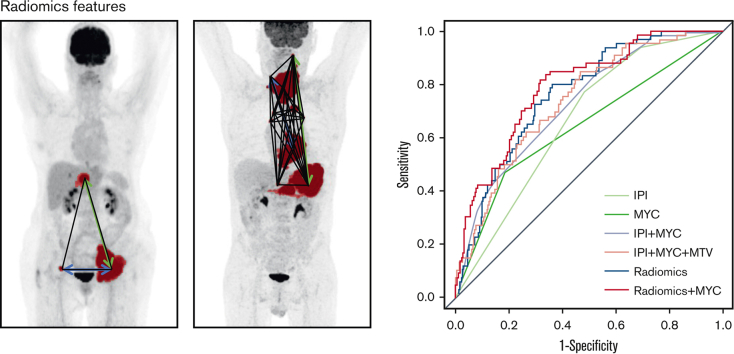
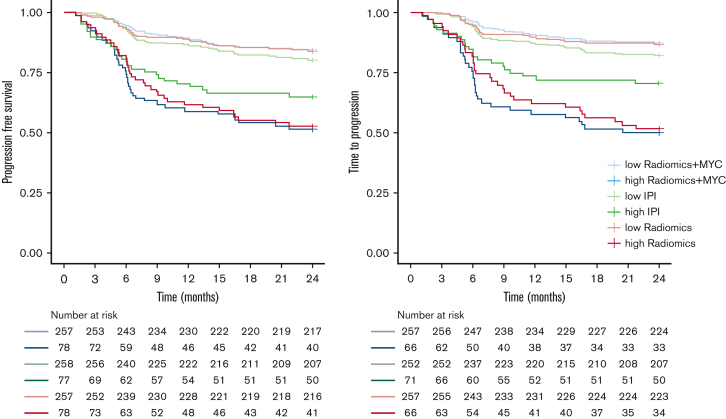
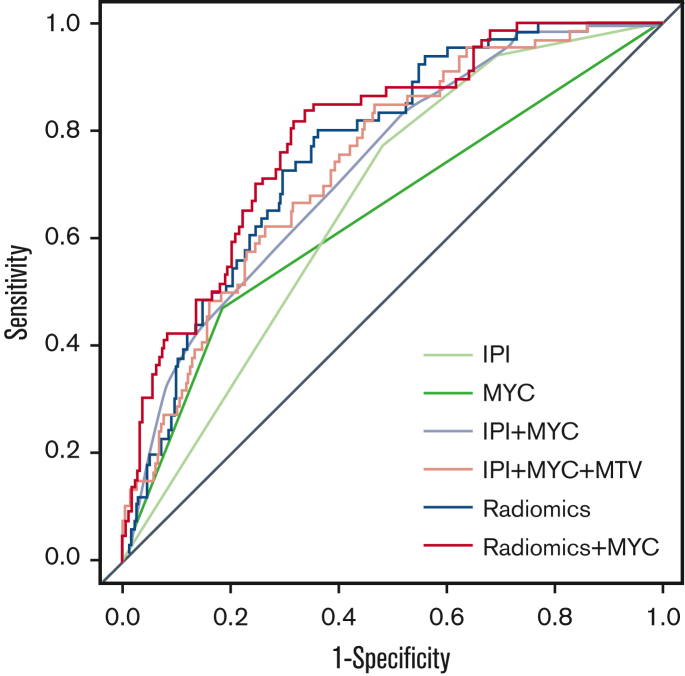
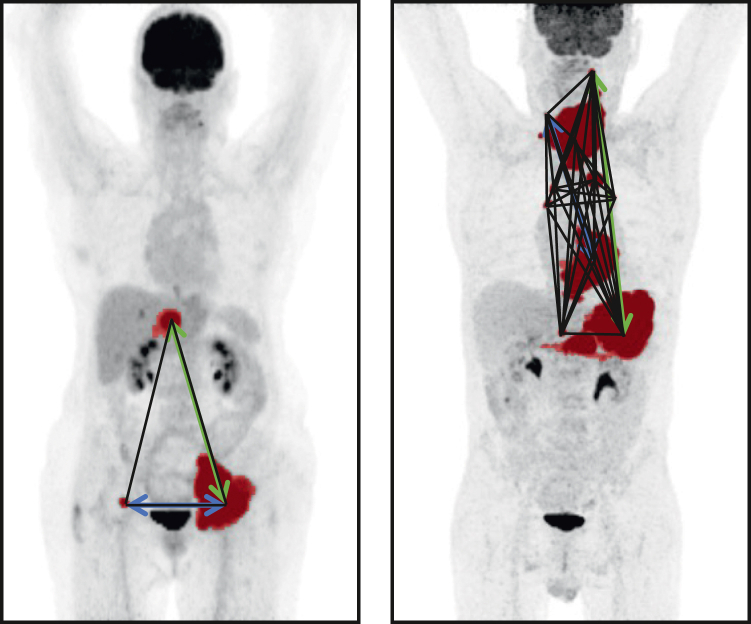
We investigated whether the outcome prediction of patients with aggressive B-cell lymphoma can be improved by combining clinical, molecular genotype, and radiomics features. MYC, BCL2, and BCL6 rearrangements were assessed using fluorescence in situ hybridization. Seventeen radiomics features were extracted from the baseline positron emission tomography-computed tomography of 323 patients, which included maximum standardized uptake value (SUVmax), SUVpeak, SUVmean, metabolic tumor volume (MTV), total lesion glycolysis, and 12 dissemination features pertaining to distance, differences in uptake and volume between lesions, respectively. Logistic regression with backward feature selection was used to predict progression after 2 years. The predictive value of (1) International Prognostic Index (IPI); (2) IPI plus MYC; (3) IPI, MYC, and MTV; (4) radiomics; and (5) MYC plus radiomics models were tested using the cross-validated area under the curve (CV-AUC) and positive predictive values (PPVs). IPI yielded a CV-AUC of 0.65 ± 0.07 with a PPV of 29.6%. The IPI plus MYC model yielded a CV-AUC of 0.68 ± 0.08. IPI, MYC, and MTV yielded a CV-AUC of 0.74 ± 0.08. The highest model performance of the radiomics model was observed for MTV combined with the maximum distance between the largest lesion and another lesion, the maximum difference in SUVpeak between 2 lesions, and the sum of distances between all lesions, yielding an improved CV-AUC of 0.77 ± 0.07. The same radiomics features were retained when adding MYC (CV-AUC, 0.77 ± 0.07). PPV was highest for the MYC plus radiomics model (50.0%) and increased by 20% compared with the IPI (29.6%). Adding radiomics features improved model performance and PPV and can, therefore, aid in identifying poor prognosis patients.
我们研究了通过结合临床、分子基因型和放射组学特征是否可以改善侵袭性 B 细胞淋巴瘤患者的预后。使用荧光原位杂交评估 MYC、BCL2 和 BCL6 重排。从 323 名患者的基线正电子发射断层扫描计算机断层扫描中提取了 17 个放射组学特征,包括最大标准化摄取值(SUVmax)、SUVpeak、SUVmean、代谢肿瘤体积(MTV)、总病变糖酵解和 12 个与距离、病变摄取和体积差异相关的弥散特征。使用向后特征选择的逻辑回归来预测 2 年后的进展。使用交叉验证曲线下面积(CV-AUC)和阳性预测值(PPV)分别测试(1)国际预后指数(IPI);(2)IPI 加 MYC;(3)IPI、MYC 和 MTV;(4)放射组学;(5)MYC 加放射组学模型的预测价值。IPI 的 CV-AUC 为 0.65±0.07,PPV 为 29.6%。IPI 加 MYC 模型的 CV-AUC 为 0.68±0.08。IPI、MYC 和 MTV 的 CV-AUC 为 0.74±0.08。放射组学模型的最佳模型性能是 MTV 与最大病变与另一个病变之间的最大距离、2 个病变之间的 SUVpeak 最大差异以及所有病变之间的距离之和相结合,其 CV-AUC 提高到 0.77±0.07。当添加 MYC 时保留了相同的放射组学特征(CV-AUC,0.77±0.07)。MYC 加放射组学模型的 PPV 最高(50.0%),与 IPI(29.6%)相比增加了 20%。添加放射组学特征可提高模型性能和 PPV,因此有助于识别预后不良的患者。