Radiology Department, Hôpital Cochin, AP-HP, 27 rue du Faubourg Saint-Jacques, 75014, Paris, France.
Internal Medicine Department, Referral Center for Rare Systemic Autoimmune Diseases of Ile de France, Hôpital Cochin, AP-HP, 27 rue du Faubourg Saint-Jacques, 75014, Paris, France.
Arthritis Res Ther. 2022 Oct 28;24(1):241. doi: 10.1186/s13075-022-02935-2.
In patients with tracheobronchial involvement, the differential diagnosis between granulomatosis with polyangiitis (GPA) and relapsing polychondritis (RP) can be challenging. The aim of this study was to describe the characteristics of airway abnormalities on chest computed tomography (CT) in patients with GPA or RP and to determine whether specific imaging criteria could be used to differentiate them.
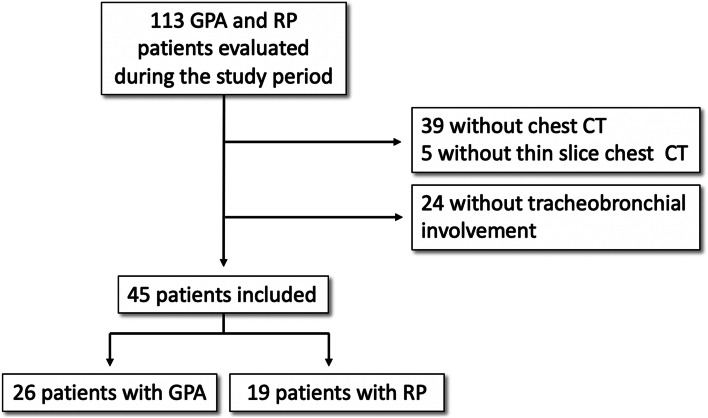
GPA and RP patients with tracheobronchial involvement referred to a national referral center from 2008 to 2020 were evaluated. Their chest CT images were reviewed by two radiologists who were blinded to the final diagnosis in order to analyze the characteristics of airway involvement. The association between imaging features and a diagnosis of GPA rather than RP was analyzed using a generalized linear regression model.
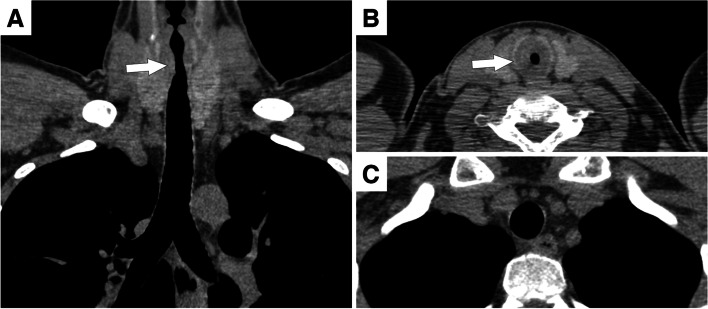
Chest CTs from 26 GPA and 19 RP patients were analyzed. Involvement of the subglottic trachea (odds ratio for GPA=28.56 [95% CI: 3.17; 847.63]; P=0.001) and extensive airway involvement (odds ratio for GPA=0.02 [95% CI: 0.00; 0.43]; P=0.008) were the two independent CT features that differentiated GPA from RP in multivariate analysis. Tracheal thickening sparing the posterior membrane was significantly associated to RP (odds ratio for GPA=0.09 [95% CI: 0.02; 0.39]; P=0.003) but only in the univariate analysis and suffered from only moderate interobserver agreement (kappa=0.55). Tracheal calcifications were also associated with RP only in the univariate analysis (odds ratio for GPA=0.21 [95% CI: 0.05; 0.78]; P=0.045).
The presence of subglottic involvement and diffuse airway involvement are the two most relevant criteria in differentiating between GPA and RP on chest CT. Although generally considered to be a highly suggestive sign of RP, posterior tracheal membrane sparing is a nonspecific and an overly subjective sign.
在气管支气管受累的患者中,区分肉芽肿性多血管炎(GPA)和复发性多软骨炎(RP)具有一定挑战性。本研究旨在描述 GPA 和 RP 患者胸部 CT 气道异常的特征,并确定是否可以使用特定的影像学标准来区分它们。
评估了 2008 年至 2020 年期间因气管支气管受累而转诊至国家转诊中心的 GPA 和 RP 患者。两名放射科医生对他们的胸部 CT 图像进行了评估,他们对最终诊断不知情,以便分析气道受累的特征。使用广义线性回归模型分析影像学特征与 GPA 诊断而非 RP 诊断之间的关联。
分析了 26 例 GPA 和 19 例 RP 患者的胸部 CT。声门下气管受累(GPA 的比值比 [OR],28.56 [95%CI:3.17;847.63];P=0.001)和广泛的气道受累(GPA 的 OR,0.02 [95%CI:0.00;0.43];P=0.008)是 GPA 与 RP 相鉴别的两个独立的 CT 特征。气管后壁不受累的气管增厚与 RP 显著相关(GPA 的 OR,0.09 [95%CI:0.02;0.39];P=0.003),但仅在单变量分析中具有中等观察者间一致性(kappa=0.55)。气管钙化也仅在单变量分析中与 RP 相关(GPA 的 OR,0.21 [95%CI:0.05;0.78];P=0.045)。
在胸部 CT 上,声门下受累和弥漫性气道受累是区分 GPA 和 RP 的两个最重要的标准。虽然通常被认为是 RP 的高度提示性标志,但气管后壁不受累是一个非特异性和过度主观的标志。