Department of Clinical Oncology, Kasr El Ainy Hospital, Cairo University, Cairo, Egypt.
Asian Pac J Cancer Prev. 2022 Oct 1;23(10):3421-3429. doi: 10.31557/APJCP.2022.23.10.3421.
The outcomes of treatment of metastatic colorectal cancer (mCRC) is still unsatisfactory. Several trials approved that, the upfront treatment with triplet regimen included fluorouracil, leucovorin, irinotecan and oxaliplatin improved the outcomes of patients with metastatic disease as compared to standard doublet regimen. The objective of our study is evaluating the impact of upfront treatment with triplet (FOLFOXIRI) regimen on both oncological outcomes (response rate and survival) and patients' tolerability in comparison to the standard doublet regimen.
We randomly enrolled 64 patients with a newly diagnosed unresectable mCRC to receive either FOLFOXIRI (experimental arm) or FOLFIRI or FOLFOX4 (control arm) biweekly up to 12 cycles. The primary endpoints are overall response rate (RR) and patients' tolerability. The secondary endpoints are the progression free and overall survival.
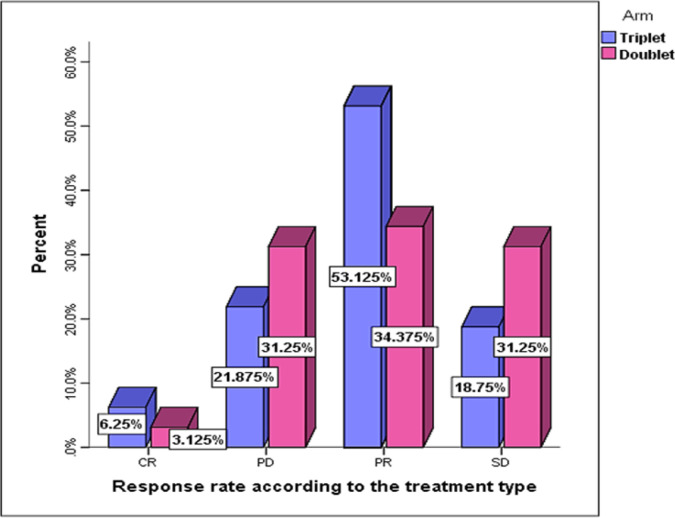
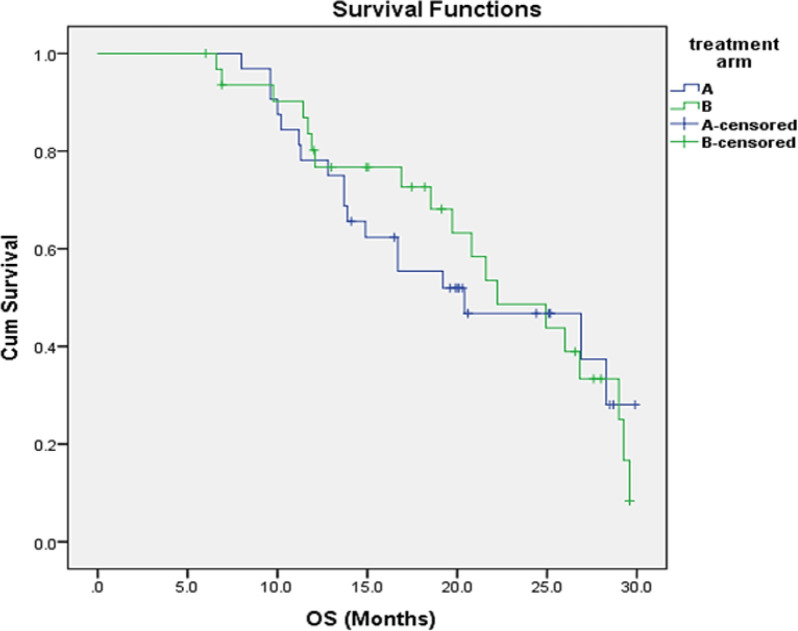
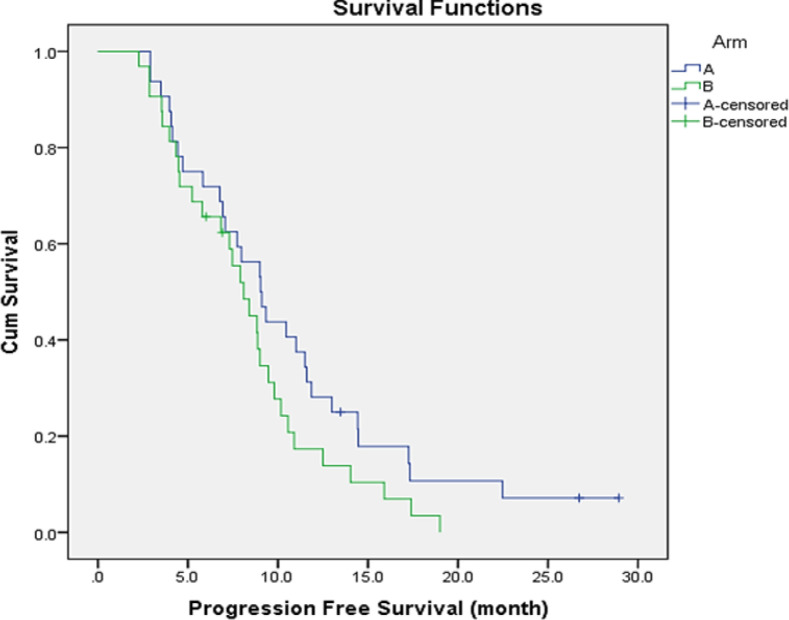
There was a significantly increase in RR (59% vs 37%) and complete remission rate (CR) (6.3% and 3.1%, respectively (P = 0.045) for the triplet therapy group compared to control group. Consequently, an increased rate of secondary resection of metastasis (21.9% vs 3.1% respectively; P=0.023). The FOLFOXIRI regimen was associated with higher rate of grade 3/4 toxicity but not statistically significant except febrile neutropenia (6.2%; P=0.03). There was numerical prolongation in the median PFS in the FOLFOXIRI group on compared to control group but not significantly (9 versus 8 months; P=0.11). The median OS was 20 and 22 months in FOLFOXIRI arm and control arm respectively with no statistically significant difference (P=0.57).
FOLFOXIRI had a higher efficacy and higher conversion rate to secondary resection over the doublet regimen as an upfront treatment option, coupled with a manageable adverse event, but failed to improve the survival outcomes.
转移性结直肠癌(mCRC)的治疗结果仍不尽如人意。几项试验证实,与标准的双联方案相比,包含氟尿嘧啶、亚叶酸钙、伊立替康和奥沙利铂的三联方案作为一线治疗可改善转移性疾病患者的预后。我们的研究目的是评估与标准双联方案相比,一线使用三联(FOLFOXIRI)方案对肿瘤学结局(缓解率和生存)和患者耐受性的影响。
我们随机招募了 64 例新诊断为不可切除的 mCRC 患者,分别接受 FOLFOXIRI(实验组)或 FOLFIRI 或 FOLFOX4(对照组)方案,每两周一次,最多 12 个周期。主要终点是总缓解率(RR)和患者的耐受性。次要终点是无进展生存期和总生存期。
与对照组相比,三联治疗组的 RR(59%比 37%)和完全缓解率(CR)(6.3%比 3.1%,P=0.045)显著增加。因此,继发转移灶切除率也显著增加(分别为 21.9%和 3.1%,P=0.023)。FOLFOXIRI 方案与更高的 3/4 级毒性发生率相关,但除发热性中性粒细胞减少症(6.2%;P=0.03)外,无统计学意义。与对照组相比,FOLFOXIRI 组的中位 PFS 略有延长,但无统计学意义(9 个月与 8 个月;P=0.11)。FOLFOXIRI 组和对照组的中位 OS 分别为 20 个月和 22 个月,无统计学差异(P=0.57)。
与双联方案相比,FOLFOXIRI 作为一线治疗选择具有更高的疗效和更高的继发转移灶切除转化率,同时具有可管理的不良反应,但未能改善生存结局。