Centre for Translational Medicine, Semmelweis University, Üllői út 26, Budapest, 1085, Hungary.
Emergency Department, Szent György University Teaching Hospital of Fejér County, Székesfehérvár, Hungary.
Intern Emerg Med. 2023 Mar;18(2):639-653. doi: 10.1007/s11739-022-03126-2. Epub 2022 Oct 31.
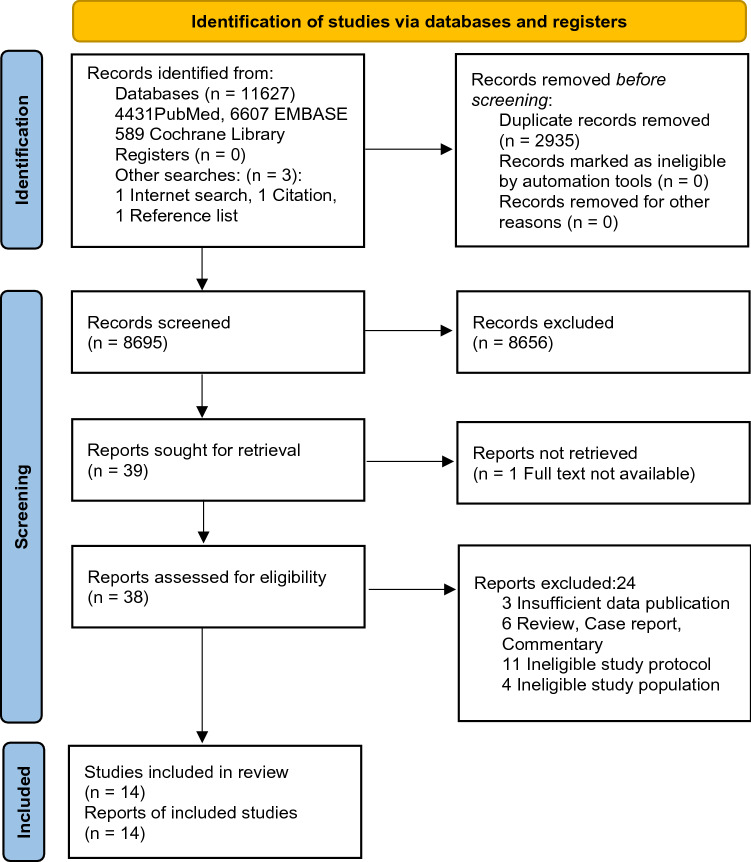
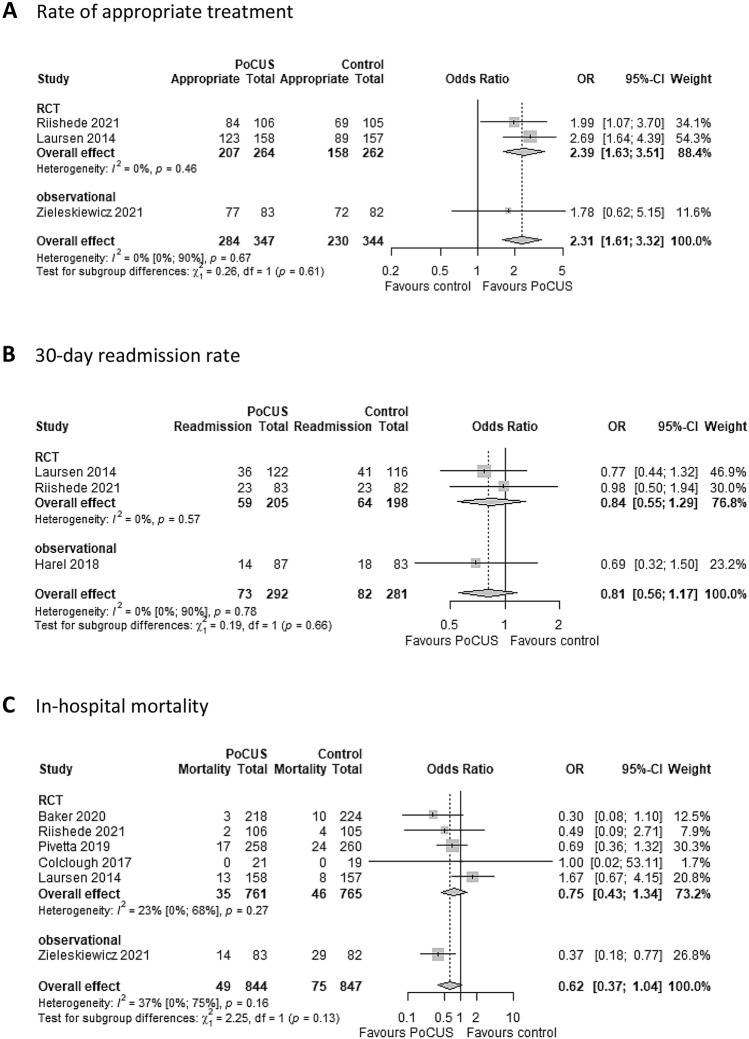
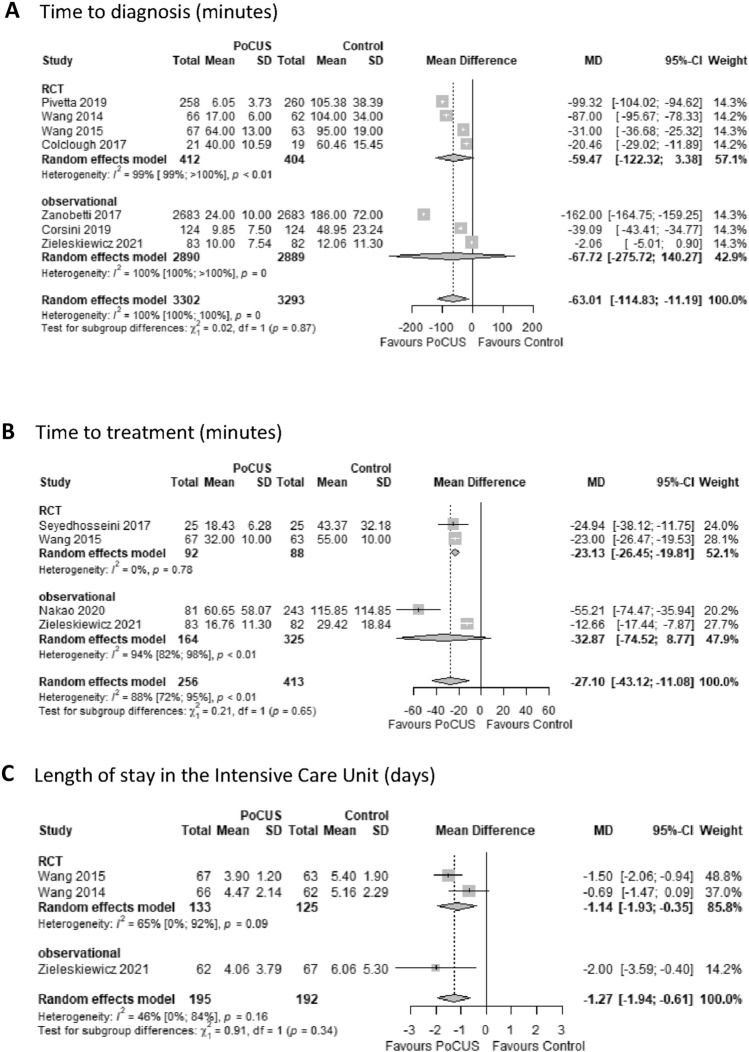
The early, appropriate management of acute onset dyspnea is important but often challenging. The aim of this study was to investigate the effects of the use of Point-of-Care Ultrasound (PoCUS) versus conventional management on clinical outcomes in patients with acute onset dyspnea. The Cochrane Library, MEDLINE, EMBASE and reference lists were searched to identify eligible trials (inception to October 14, 2021). There were no language restrictions. Randomized controlled trials (RCTs), and prospective and retrospective cohort studies that compared PoCUS with conventional diagnostic modalities (controls) in patients with acute onset dyspnea were included. Two independent reviewers extracted data and assessed the risk of bias. Disagreements were resolved by consensus. The primary study outcomes were time to diagnosis, time to treatment, and length of stay (LOS). Secondary outcomes included rate of appropriate treatment, 30-day re-admission rate, and mortality. We included eight RCTs and six observational studies with a total of 5393 participants. Heterogeneity across studies was variable (from low to considerable), with overall low or moderate study quality and low or moderate risk of bias (except one article with serious risk of bias). Time to diagnosis (mean difference [MD], - 63 min; 95% CI, - 115 to - 11 min] and time to treatment (MD, - 27 min; 95% CI - 43 to - 11 min) were significantly shorter in the PoCUS group. In-hospital LOS showed no differences between the two groups, but LOS in the Intensive Care Unit (MD, - 1.27 days; - 1.94 to - 0.61 days) was significantly shorter in the PoCUS group. Patients in the PoCUS group showed significantly higher odds of receiving appropriate therapy compared to controls (odds ratio [OR], 2.31; 95% CI, 1.61-3.32), but there was no significant effect on 30-day re-admission rate and in-hospital or 30-day mortality. Our results indicate that PoCUS use contributes to early diagnosis and better outcomes compared to conventional methods in patients admitted with acute onset dyspnea.
急性发作性呼吸困难的早期适当管理很重要,但往往具有挑战性。本研究旨在探讨床边超声(PoCUS)与常规管理对急性发作性呼吸困难患者临床结局的影响。从 Cochrane 图书馆、MEDLINE、EMBASE 和参考文献中检索到符合条件的试验(从开始到 2021 年 10 月 14 日)。没有语言限制。纳入了比较急性发作性呼吸困难患者 PoCUS 与常规诊断方法(对照组)的随机对照试验(RCT)、前瞻性和回顾性队列研究。两名独立的审查员提取数据并评估偏倚风险。意见分歧通过协商解决。主要研究结果是诊断时间、治疗时间和住院时间(LOS)。次要结果包括适当治疗率、30 天再入院率和死亡率。我们纳入了 8 项 RCT 和 6 项观察性研究,共有 5393 名参与者。研究之间的异质性各不相同(从低到高),总体研究质量低或中等,偏倚风险低或中等(除了一篇文章存在严重的偏倚风险)。PoCUS 组的诊断时间(平均差 [MD],-63 分钟;95%CI,-115 至-11 分钟)和治疗时间(MD,-27 分钟;95%CI,-43 至-11 分钟)明显缩短。两组患者的住院 LOS 无差异,但 PoCUS 组 ICU 住院 LOS 明显缩短(MD,-1.27 天;-1.94 至-0.61 天)。与对照组相比,PoCUS 组患者接受适当治疗的可能性明显更高(优势比 [OR],2.31;95%CI,1.61-3.32),但对 30 天再入院率、住院或 30 天死亡率无显著影响。我们的研究结果表明,与常规方法相比,PoCUS 的使用可以在急性发作性呼吸困难患者中实现早期诊断和更好的结局。