Le Thu-Thao, Huang Benjamin, Pua Chee Jian, Tornekar Vineet, Schumacher-Maurer Annette, Toh Desiree-Faye, Bryant Jennifer, Ang Briana, Corden Ben, Prasad Sanjay K, Tang Hak-Chiaw, Cook Stuart A, Chin Calvin W L
Department of Cardiology, National Heart Centre Singapore, Singapore.
Cardiovascular Academic Clinical Program, Duke NUS Medical School, Singapore.
JACC Asia. 2021 Sep 21;1(2):218-226. doi: 10.1016/j.jacasi.2021.07.001. eCollection 2021 Sep.
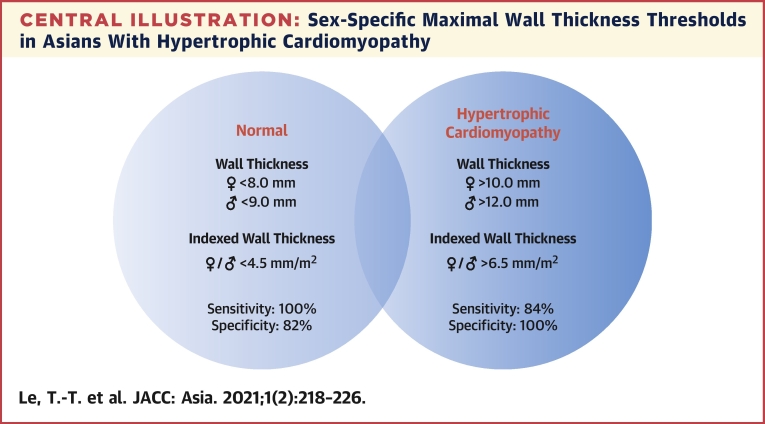
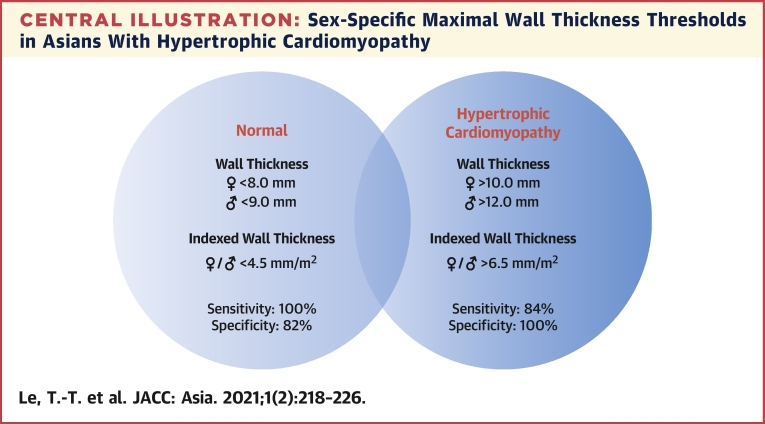
Hypertrophic cardiomyopathy (HCM) is defined as left ventricular end-diastolic maximal wall thickness (WT) ≥15.0 mm, without accounting for ethnicity, sex, and body size. It is well-established that Asians have smaller hearts than do Caucasians.
This study aims to examine the implications of this single absolute WT threshold on the diagnosis of HCM in Asians.
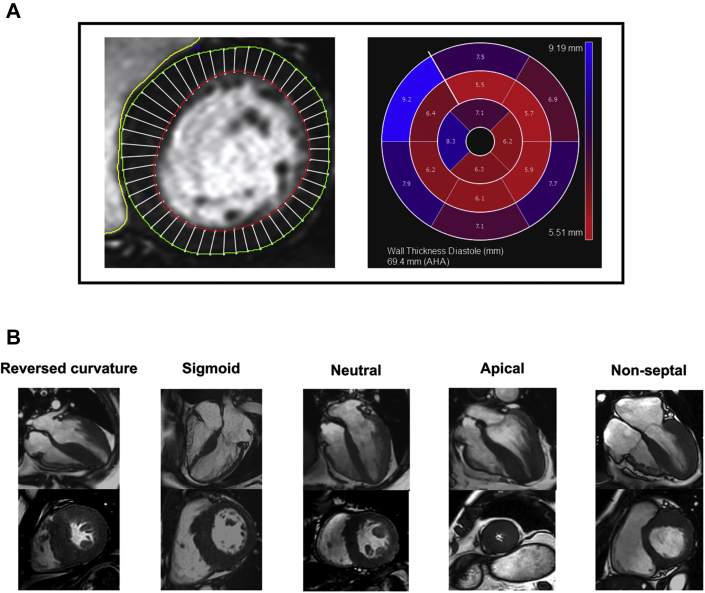
The study consisted of 360 healthy volunteers (male: n = 174; age: 50 ± 12 years) and 114 genetically characterized patients with HCM (male: n = 83; age: 52 ± 13 years; genotype-positive, n = 39). All participants underwent cardiovascular magnetic resonance. WT was measured semiautomatically at end-diastole according to the standard 16 myocardial segments.
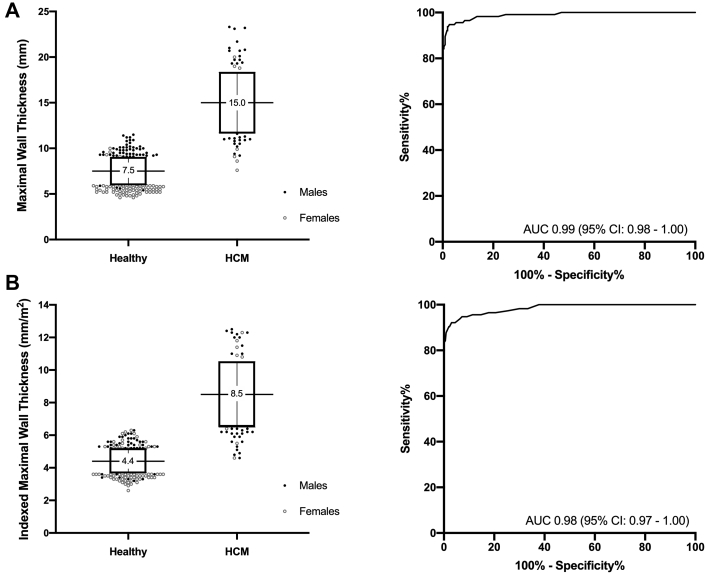
Healthy male volunteers had increased WT compared with that of female volunteers (8.4 ± 1.2 mm vs 6.6 ± 1.1 mm, respectively; 0.001). Conversely, WT was similar between male and female patients with HCM (15.2 ± 3.4 mm vs 14.7 ± 3.0 mm, respectively; 0.484) and between those with and without a pathogenic gene variant 0.828). Using the recommended diagnostic threshold of 15.0 mm, 56 patients with HCM had WT <15.0 mm and no healthy volunteers had WT >15.0 mm (specificity of 100% and sensitivity of 51%). Lowering WT thresholds to 10.0 mm in female patients and 12.0 mm in male patients did not affect specificity (100%) but significantly improved sensitivity (84%). Despite lower left ventricular mass, female patients with HCM demonstrated more features of adverse cardiac remodeling than did male patients: increased myocardial fibrosis, higher asymmetric ratio, and disproportionately worse myocardial strain.
The study highlights cautious application of guideline-recommended WT to diagnose HCM in Asians. Lowering WT to account for ethnicity and sex improves diagnostic sensitivity without compromising specificity.
肥厚型心肌病(HCM)定义为左心室舒张末期最大壁厚(WT)≥15.0mm,不考虑种族、性别和体型。众所周知,亚洲人的心脏比白种人小。
本研究旨在探讨这一单一绝对WT阈值对亚洲人HCM诊断的影响。
该研究包括360名健康志愿者(男性:n = 174;年龄:50±12岁)和114名经基因特征分析的HCM患者(男性:n = 83;年龄:52±13岁;基因阳性,n = 39)。所有参与者均接受了心血管磁共振检查。根据标准的16个心肌节段,在舒张末期半自动测量WT。
健康男性志愿者的WT高于女性志愿者(分别为8.4±1.2mm和6.6±1.1mm;P<0.001)。相反,HCM男性和女性患者之间的WT相似(分别为15.2±3.4mm和14.7±3.0mm;P = 0.484),有和没有致病基因变异的患者之间也是如此(P = 0.828)。使用推荐的诊断阈值15.0mm时,56例HCM患者的WT<15.0mm,没有健康志愿者的WT>15.0mm(特异性为100%,敏感性为51%)。将女性患者的WT阈值降至10.0mm,男性患者降至12.0mm,不影响特异性(100%),但显著提高了敏感性(84%)。尽管左心室质量较低,但HCM女性患者比男性患者表现出更多不良心脏重塑特征:心肌纤维化增加、不对称率更高以及心肌应变异常严重。
该研究强调在亚洲人HCM诊断中谨慎应用指南推荐的WT。根据种族和性别降低WT可提高诊断敏感性而不影响特异性。