Patel Mital, Gbadegesin Rasheed A
Department of Pediatrics, Division of Pediatric Nephrology, Duke University, Durham, NC, United State.
Front Pediatr. 2022 Oct 21;10:1039024. doi: 10.3389/fped.2022.1039024. eCollection 2022.
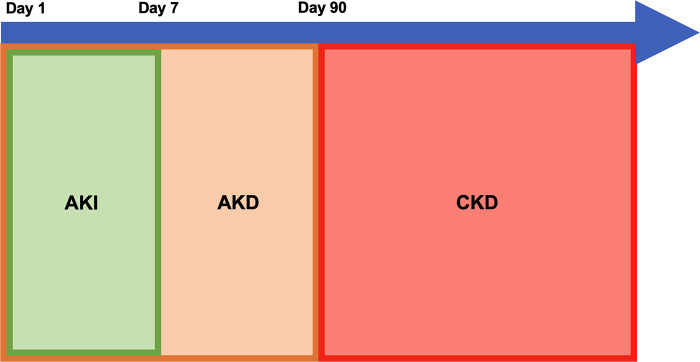
Acute kidney injury (AKI) affects a large proportion of hospitalized children and increases morbidity and mortality in this population. Initially thought to be a self-limiting condition with uniformly good prognosis, we now know that AKI can persist and progress to acute kidney disease (AKD) and chronic kidney disease (CKD). AKI is presently categorized by stage of injury defined by increase in creatinine, decrease in eGFR, or decrease in urine output. These commonly used biomarkers of acute kidney injury do not change until the injury is well established and are unable to detect early stage of the disease when intervention is likely to reverse injury. The kidneys have the ability to compensate and return serum creatinine to a normal or baseline level despite nephron loss in the setting of AKI possibly masking persistent dysfunction. Though these definitions are important, classifying children by their propensity for progression to AKD and CKD and defining these risk strata by other factors besides creatinine may allow for better prognosis driven discussion, expectation setting, and care for our patients. In order to develop a classification strategy, we must first be able to recognize children who are at risk for AKD and CKD based on modifiable and non-modifiable factors as well as early biomarkers that identify their risk of persistent injury. Prevention of initial injury, prompt evaluation and treatment if injury occurs, and mitigating further injury during the recovery period may be important factors in decreasing risk of AKD and CKD after AKI. This review will cover presently used definitions of AKI, AKD, and CKD, recent findings in epidemiology and risk factors for AKI to AKD to CKD progression, novel biomarkers for early identification of AKI and AKI that may progress to CKD and future directions for improving outcome in children with AKI.
急性肾损伤(AKI)影响着很大一部分住院儿童,并增加了这一人群的发病率和死亡率。最初认为这是一种具有一致良好预后的自限性疾病,而现在我们知道AKI可能会持续并进展为急性肾脏病(AKD)和慢性肾脏病(CKD)。目前,AKI是根据肌酐升高、估算肾小球滤过率(eGFR)降低或尿量减少所定义的损伤阶段进行分类的。这些常用的急性肾损伤生物标志物在损伤确立之前不会发生变化,并且在疾病早期阶段、干预有可能逆转损伤时无法检测到。尽管在AKI情况下存在肾单位丢失,但肾脏有能力进行代偿并使血清肌酐恢复到正常或基线水平,这可能掩盖了持续存在的功能障碍。虽然这些定义很重要,但根据儿童进展为AKD和CKD的倾向对其进行分类,并通过肌酐以外的其他因素来定义这些风险分层,可能有助于进行以更好预后为导向的讨论、设定预期以及为我们的患者提供护理。为了制定一种分类策略,我们首先必须能够根据可改变和不可改变的因素以及识别其持续损伤风险的早期生物标志物,识别出有AKD和CKD风险的儿童。预防初始损伤、在损伤发生时及时评估和治疗,以及在恢复期减轻进一步损伤,可能是降低AKI后发生AKD和CKD风险的重要因素。本综述将涵盖目前使用的AKI、AKD和CKD的定义、AKI至AKD至CKD进展的流行病学和危险因素的最新发现、用于早期识别AKI以及可能进展为CKD的AKI的新型生物标志物,以及改善AKI患儿预后的未来方向。