Hagens Marinus J, Noordzij M Arjen, Mazel Jan Willem, Jager Auke, Boellaard Thierry N, Tielbeek Jeroen A W, Henebiens Margot, Schoots Ivo G, van Leeuwen Pim J, van der Poel Henk G, Rynja Sybren P
Department of Urology, Amsterdam UMC Location Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Department of Urology, Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital (NCI-AVL), Amsterdam, The Netherlands.
Eur Urol Open Sci. 2022 Aug 2;43:68-73. doi: 10.1016/j.euros.2022.07.006. eCollection 2022 Sep.
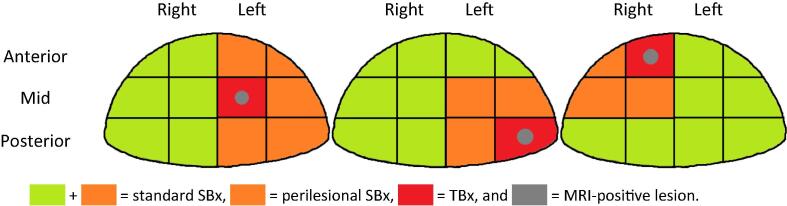
Considering that most men benefit diagnostically from increased sampling of index lesions, limiting systematic biopsy (SBx) to the region around the index lesion could potentially minimize overdetection while maintaining the detection of clinically significant prostate cancer (csPCa).
To evaluate the diagnostic performance of a hypothetical magnetic resonance imaging (MRI)-directed targeted-plus-perilesional biopsy approach.
This single-center, retrospective analysis of prospectively generated data included all biopsy-naïve men with unilateral MRI-positive lesions (Prostate Imaging Reporting and Data System category ≥3), undergoing both MRI-directed targeted biopsies and SBx. Grade group 2-5 cancers were considered csPCa.
The diagnostic performance of a targeted-plus-perilesional biopsy approach was compared with that of a targeted-plus-systematic biopsy approach. The primary outcome was the detection of csPCa. Secondary outcomes included the detection of clinically insignificant prostate cancer (ciPCa) and the number of total biopsy cores.
A total of 235 men were included in the analysis; csPCa and ciPCa were detected, respectively, in 95 (40.4%) and 86 (36.6%) of these 235 men. A targeted-plus-perilesional biopsy approach would have detected 92/95 (96.8%; 95% confidence interval [CI] 91.0-99.3%) csPCa cases. At the same time, detection of systematically found ciPCa would be reduced by 11/86 (12.8%; 95% CI 6.6-21.7%). If a targeted-plus-perilesional biopsy approach would have been performed, the number of biopsy cores per patient would have been reduced significantly (a mean difference of 5.2; 95% CI 4.9-5.6, < 0.001).
An MRI-directed targeted-plus-perilesional biopsy approach detected almost all csPCa cases, while limiting overdiagnosis and reducing the number of biopsy cores. Prospective clinical trials are needed to substantiate the withholding of nonperilesional SBx in men with unilateral lesion(s) on MRI.
Limiting systematic biopsies to the proximity of the suspicious area on magnetic resonance imaging helps detect an equivalent number of aggressive cancers and fewer indolent cancers. These findings may help patients and physicians choose the best biopsy approach.
鉴于大多数男性通过增加对索引病变的采样在诊断上获益,将系统活检(SBx)局限于索引病变周围区域可能在维持对临床显著前列腺癌(csPCa)检测的同时将过度诊断降至最低。
评估一种假设的磁共振成像(MRI)引导的靶向加病变周围活检方法的诊断性能。
设计、设置和参与者:这项对前瞻性收集数据的单中心回顾性分析纳入了所有未经活检、有单侧MRI阳性病变(前列腺影像报告和数据系统类别≥3)且接受了MRI引导的靶向活检和SBx的男性。2-5级癌症被视为csPCa。
将靶向加病变周围活检方法的诊断性能与靶向加系统活检方法的进行比较。主要结果是csPCa的检测。次要结果包括临床意义不显著的前列腺癌(ciPCa)的检测以及活检针芯总数。
共有235名男性纳入分析;在这235名男性中,分别检测到95例(40.4%)csPCa和86例(36.6%)ciPCa。靶向加病变周围活检方法本可检测到92/95(96.8%;95%置信区间[CI]91.0-99.3%)的csPCa病例。同时,系统发现的ciPCa的检测将减少11/86(12.8%;95%CI 6.6-21.7%)。如果采用靶向加病变周围活检方法,每位患者的活检针芯数量将显著减少(平均差异为5.2;95%CI 4.9-5.6,<0.001)。
MRI引导的靶向加病变周围活检方法检测到了几乎所有的csPCa病例,同时限制了过度诊断并减少了活检针芯数量。需要进行前瞻性临床试验以证实对于MRI有单侧病变的男性不进行病变周围外的SBx。
将系统活检局限于磁共振成像上可疑区域附近有助于检测出数量相当的侵袭性癌症和更少的惰性癌症。这些发现可能有助于患者和医生选择最佳活检方法。