Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark
Department of Cardiology, Rigshospitalet, Copenhagen, Denmark.
Heart. 2022 Nov 10;108(23):1895-1903. doi: 10.1136/heartjnl-2022-321204.
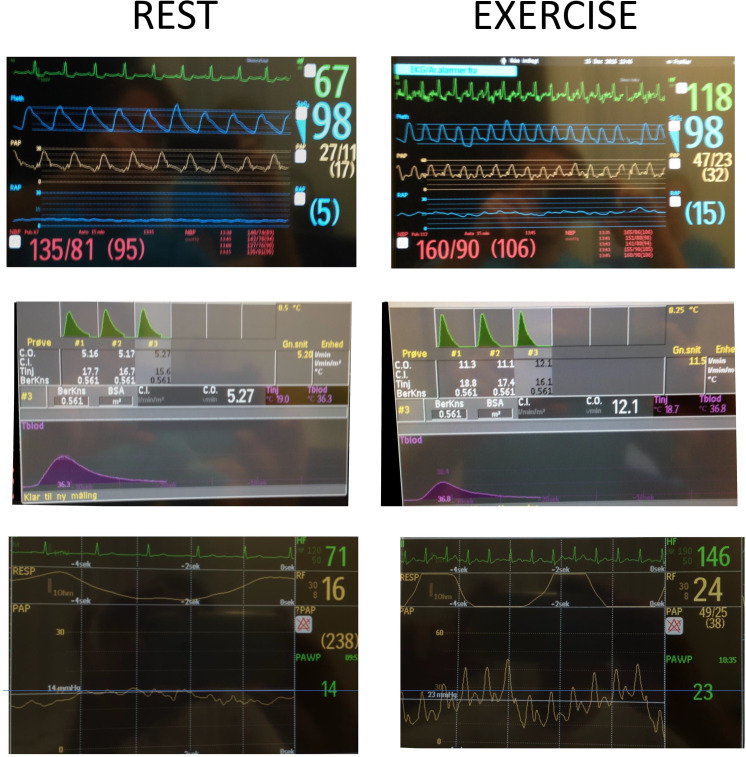
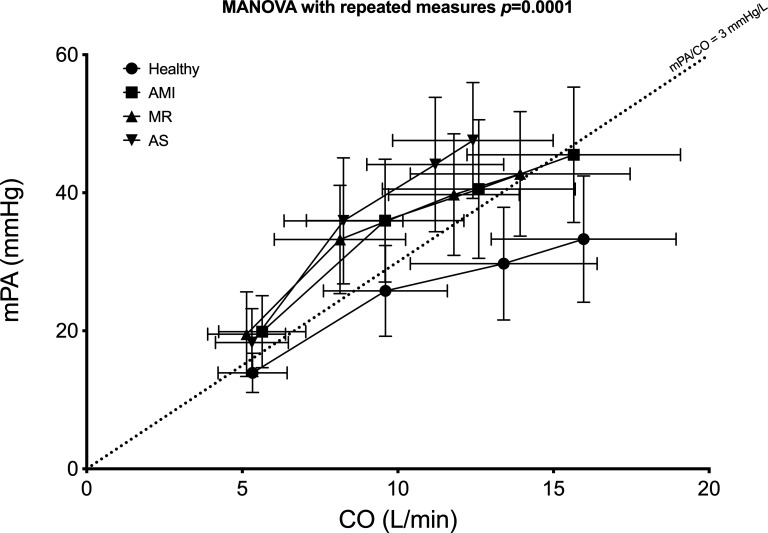
Haemodynamic exercise testing is important for evaluating patients with dyspnoea on exertion and preserved ejection fraction. Despite very different pathologies, patients with pressure (aortic stenosis (AS)) and volume (mitral regurgitation (MR)) overload and diastolic dysfunction after recent acute myocardial infarction (AMI) reach similar filling pressure levels with exercise. The pressure-flow relationships (the association between change in cardiac output (∆CO) and change in pulmonary arterial wedge pressure (∆PAWP) may provide insight into haemodynamic adaptation to exercise in these groups.
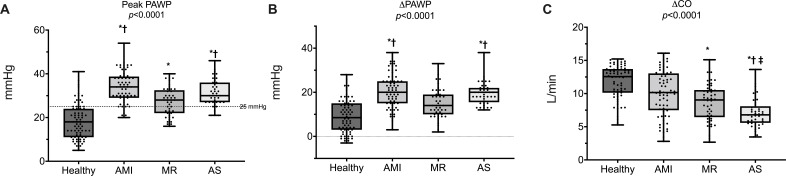
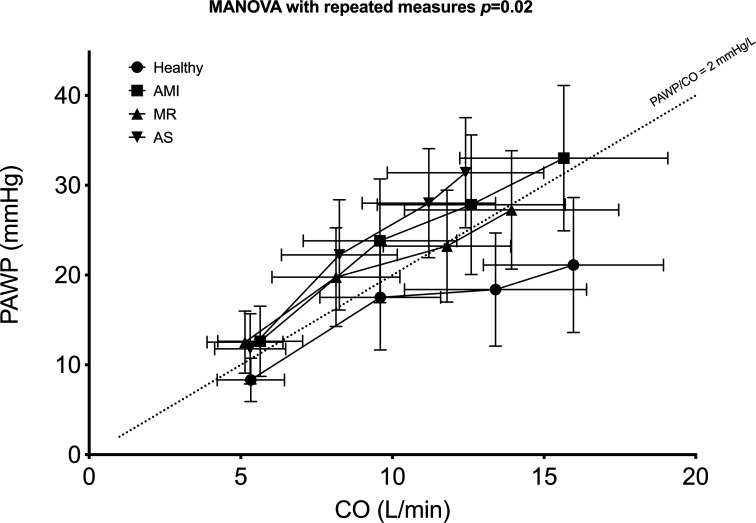
One hundred sixty-eight subjects aged >50 years with a left ventricular ejection fraction of ≥50% underwent invasive exercise testing. They were enrolled in four different studies: AS (40 patients), AMI (52 patients), MR (43 patients) and 33 healthy subjects. Haemodynamic data were measured at rest, at 25 W, 75 W and at peak exercise. In all groups, PAWP increased with exercise. The greatest increase was observed in patients with AMI (from 12.7±3.9 mm Hg to 33.1±8.2 mm Hg, p<0.0001) and patients with AS (from 11.8±3.9 mm Hg to 31.4±6.1 mm Hg, p<0.0001), and the smallest was observed in healthy subjects (from 8.3±2.4 mm Hg to 21.1±7.5 mm Hg, p<0.0001). In all groups, the relative pressure increase was greatest at the beginning of the exercise. CO increased most in healthy patients (from 5.3±1.1 to 16.0±3.0 L/min, p<0.0001) and least in patients with AS (from 5.3±1.2 L/min to 12.4±2.6 L/min, p<0.0001). The pressure-flow relationships (∆PAWP/∆CO) and differed among groups (p0.02). In all groups, the pressure-flow relationship was steepest in the initial phase of the exercise test. The AMI and AS groups (2.3±1.2 mm Hg/L/min and 3.0±1.3 mm Hg/L/min, AMI and AS, respectively) had the largest overall pressure-flow relationship; the healthy group had the smallest initially and at peak exercise (1.3±1.1 mm Hg/L/min) followed by MR group (1.9±1.4 mm Hg/L/min).
The pressure-flow relationship was steepest in the initial phase of the exercise test in all groups. The pressure-flow relationship differs between groups.
NCT01974557, NCT01046838, NCT02961647 and NCT02395107.
血流动力学运动试验对于评估运动时呼吸困难和射血分数保留的患者非常重要。尽管存在非常不同的病理学,但近期急性心肌梗死(AMI)后压力(主动脉瓣狭窄(AS))和容量(二尖瓣反流(MR))过载以及舒张功能障碍的患者在运动时达到相似的充盈压水平。压力-流量关系(心输出量变化与肺动脉楔压变化之间的关系(∆CO 和 ∆PAWP)可能有助于深入了解这些组对运动的血液动力学适应。
168 名年龄>50 岁且左心室射血分数≥50%的患者接受了侵入性运动测试。他们被纳入四项不同的研究:AS(40 例)、AMI(52 例)、MR(43 例)和 33 名健康受试者。在休息、25 W、75 W 和峰值运动时测量血流动力学数据。在所有组中,PAWP 在运动时增加。观察到 AMI 患者(从 12.7±3.9 mm Hg 增加到 33.1±8.2 mm Hg,p<0.0001)和 AS 患者(从 11.8±3.9 mm Hg 增加到 31.4±6.1 mm Hg,p<0.0001)的增加最大,而健康受试者的增加最小(从 8.3±2.4 mm Hg 增加到 21.1±7.5 mm Hg,p<0.0001)。在所有组中,压力在运动开始时增加最大。CO 在健康患者中增加最多(从 5.3±1.1 L/min 增加到 16.0±3.0 L/min,p<0.0001),在 AS 患者中增加最少(从 5.3±1.2 L/min 增加到 12.4±2.6 L/min,p<0.0001)。压力-流量关系(∆PAWP/∆CO)在组间存在差异(p<0.02)。在所有组中,压力-流量关系在运动试验的初始阶段最为陡峭。AMI 和 AS 组(分别为 2.3±1.2 mm Hg/L/min 和 3.0±1.3 mm Hg/L/min)具有最大的整体压力-流量关系;健康组在初始阶段和峰值运动时最小(1.3±1.1 mm Hg/L/min),其次是 MR 组(1.9±1.4 mm Hg/L/min)。
在所有组中,压力-流量关系在运动试验的初始阶段最为陡峭。各组之间的压力-流量关系不同。
NCT01974557、NCT01046838、NCT02961647 和 NCT02395107。