Assistance Publique - Hôpitaux de Paris, Service de Médecine Intensive Réanimation, Hôpital Tenon, APHP, Sorbonne Université, 4 Rue de la Chine, 75020, Paris, France.
Assistance Publique - Hôpitaux de Paris, Service de Médecine Intensive Réanimation, Hôpital Saint-Antoine, Sorbonne Université, Paris, France.
Crit Care. 2022 Nov 12;26(1):350. doi: 10.1186/s13054-022-04228-1.
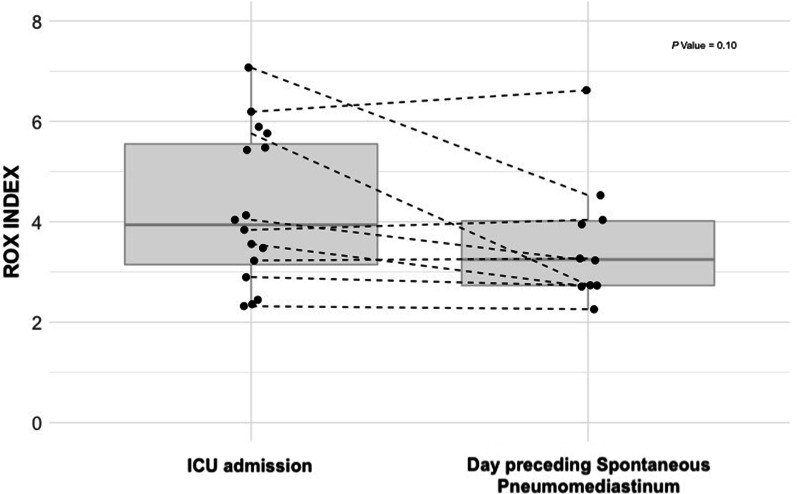
Spontaneous pneumomediastinum (SP) has been described early during the COVID-19 pandemic in large series of patients with severe pneumonia, but most patients were receiving invasive mechanical ventilation (IMV) at the time of SP diagnosis. In this retrospective multicenter observational study, we aimed at describing the prevalence and outcomes of SP during severe COVID-19 with pneumonia before any IMV, to rule out mechanisms induced by IMV in the development of pneumomediastinum.Among 549 patients, 21 patients (4%) developed a SP while receiving non-invasive respiratory support, after a median of 6 days [4-12] from ICU admission. The proportion of patients requiring IMV was similar. However, the time to tracheal intubation was longer in patients with SP (6 days [5-13] vs. 2 days [1-4]; P = 0.00002), with a higher first-line use of non-invasive ventilation (n = 11; 52% vs. n = 150; 28%; P = 0.02). The 21 patients who developed a SP had persisting signs of severe lung disease and respiratory failure with lower ROX index between ICU admission and occurrence of SP (3.94 [3.15-5.55] at admission vs. 3.25 [2.73-4.02] the day preceding SP; P = 0.1), which may underline potential indirect signals of Patient-self inflicted lung injury (P-SILI).In this series of critically ill COVID-19 patients, the prevalence of SP without IMV was not uncommon, affecting 4% of patients. They received more often vasopressors and had a longer ICU length of stay, as compared with their counterparts. One pathophysiological mechanism may potentially be carried out by P-SILI related to a prolonged respiratory failure, as underlined by a delayed use of IMV and the evolution of the ROX index between ICU admission and the day preceding SP.
自发性纵隔气肿(SP)在大系列严重肺炎患者中曾在 COVID-19 大流行早期被描述,但大多数患者在 SP 诊断时正在接受有创机械通气(IMV)。在这项回顾性多中心观察性研究中,我们旨在描述在没有任何 IMV 的情况下,患有严重 COVID-19 合并肺炎时 SP 的患病率和结局,以排除 IMV 引起的机制在纵隔气肿发展中的作用。在 549 名患者中,21 名患者(4%)在接受无创呼吸支持时发生了 SP,在 ICU 入院后中位数为 6 天[4-12]。需要 IMV 的患者比例相似。然而,SP 患者的气管插管时间更长(6 天[5-13]与 2 天[1-4];P = 0.00002),一线使用无创通气的比例更高(n = 11;52%与 n = 150;28%;P = 0.02)。发生 SP 的 21 名患者持续存在严重肺部疾病和呼吸衰竭的迹象,ROX 指数在 ICU 入院和 SP 发生之间降低(入院时为 3.94[3.15-5.55],SP 前一天为 3.25[2.73-4.02];P = 0.1),这可能突出了潜在的患者自我造成的肺损伤(P-SILI)的间接信号。在这一系列重症 COVID-19 患者中,无 IMV 的 SP 患病率并不少见,影响了 4%的患者。与他们的对照组相比,他们接受血管加压药的频率更高,并且 ICU 住院时间更长。一种潜在的病理生理机制可能是由与延长的呼吸衰竭相关的 P-SILI 引起的,这一点可以从 IMV 的延迟使用和 ROX 指数在 ICU 入院和 SP 前一天之间的演变中得到强调。