Marincowitz Carl, Hodkinson Peter, McAlpine David, Fuller Gordon, Goodacre Steve, Bath Peter A, Sbaffi Laura, Hasan Madina, Omer Yasein, Wallis Lee
Centre for Urgent and Emergency Care Research (CURE), Health Services Research School of Health and Related Research, University of Sheffield, Regent Court, 30 Regent Street, Sheffield, S1 4DA, UK.
Division of Emergency Medicine, University of Cape Town, F51 Old Main Building, Groote Schuur Hospital, Observatory, Cape Town.
medRxiv. 2022 Nov 7:2022.11.06.22281986. doi: 10.1101/2022.11.06.22281986.
Uneven vaccination and less resilient health care systems mean hospitals in LMICs are at risk of being overwhelmed during periods of increased COVID-19 infection. Risk-scores proposed for rapid triage of need for admission from the emergency department (ED) have been developed in higher-income settings during initial waves of the pandemic.
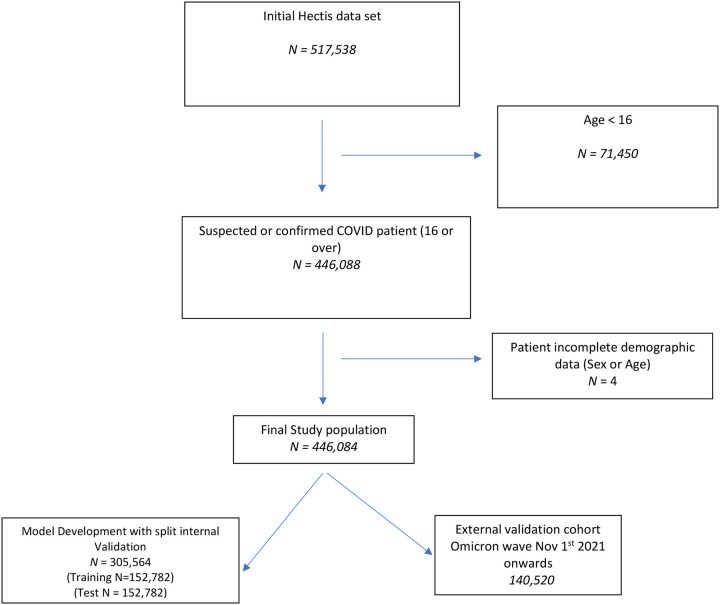
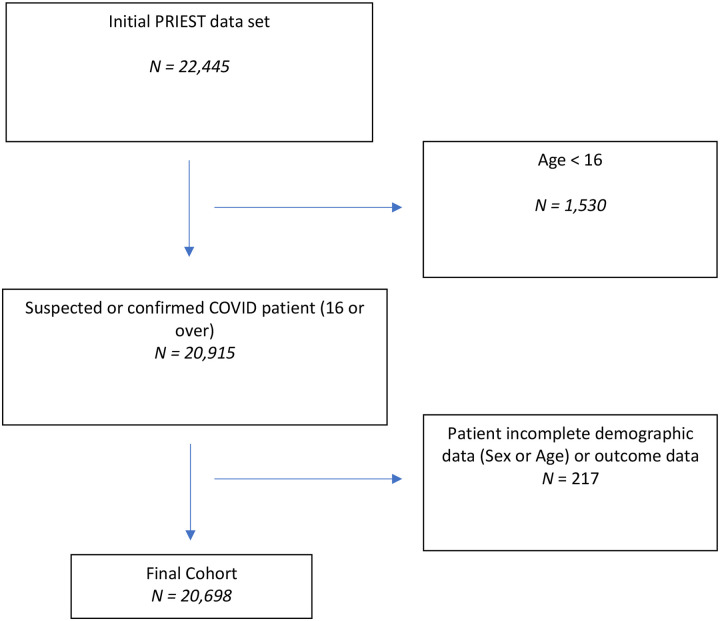
Routinely collected data for public hospitals in the Western Cape, South Africa from the 27 August 2020 to 11 March 2022 were used to derive a cohort of 446,084 ED patients with suspected COVID-19. The primary outcome was death or ICU admission at 30 days. The cohort was divided into derivation and Omicron variant validation sets. We developed the LMIC-PRIEST score based on the coefficients from multivariable analysis in the derivation cohort and existing triage practices. We externally validated accuracy in the Omicron period and a UK cohort.
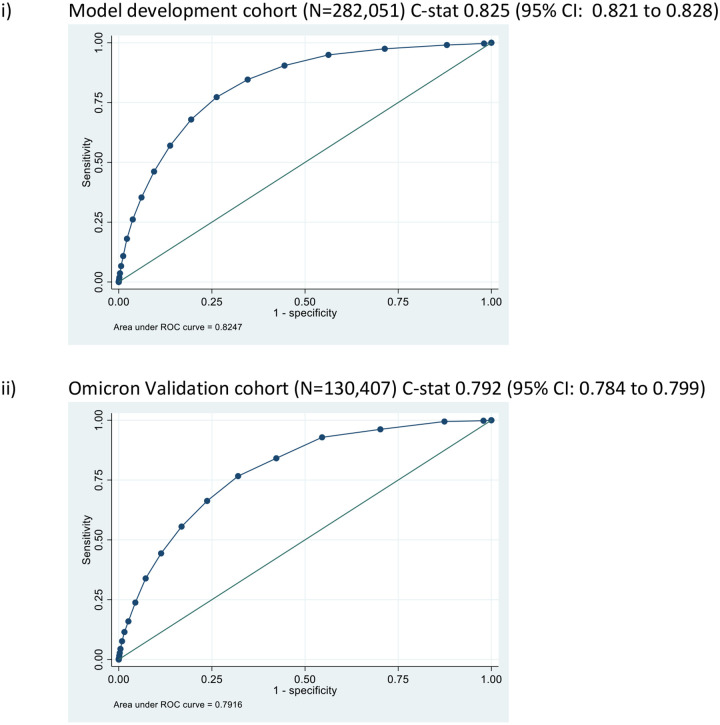
We analysed 305,564, derivation 140,520 Omicron and 12,610 UK validation cases. Over 100 events per predictor parameter were modelled. Multivariable analyses identified eight predictor variables retained across models. We used these findings and clinical judgement to develop a score based on South African Triage Early Warning Scores and also included age, sex, oxygen saturation, inspired oxygen, diabetes and heart disease. The LMIC-PRIEST score achieved C-statistics: 0.82 (95% CI: 0.82 to 0.83) development cohort; 0.79 (95% CI: 0.78 to 0.80) Omicron cohort; and 0.79 (95% CI: 0.79 to 0.80) UK cohort. Differences in prevalence of outcomes led to imperfect calibration in external validation. However, use of the score at thresholds of three or less would allow identification of very low-risk patients (NPV ≥0.99) who could be rapidly discharged using information collected at initial assessment.
The LMIC-PRIEST score shows good discrimination and high sensitivity at lower thresholds and can be used to rapidly identify low-risk patients in LMIC ED settings.
Uneven vaccination in low- and middle-income countries (LMICs) coupled with less resilient health care provision mean that emergency health care systems in LMICs may still be at risk of being overwhelmed during periods of increased COVID-19 infection.Risk-stratification scores may help rapidly triage need for hospitalisation. However, those proposed for use in the ED for patients with suspected COVID-19 have been developed and validated in high-income settings.
The LMIC-PRIEST score has been robustly developed using a large routine dataset from the Western Cape, South Africa and is directly applicable to existing triage practices in LMICs.External validation across both income settings and COVID-19 variants showed good discrimination and high sensitivity (at lower thresholds) to a composite outcome indicating need for inpatient admission from the ED.
Use of the LMIC-PRIEST score at thresholds of three or less would allow identification of very low-risk patients (negative predictive value ≥0.99) across all settings assessedDuring periods of increased demand, this could allow the rapid identification and discharge of patients from the ED using information collected at initial assessment.
疫苗接种不均衡以及医疗保健系统韧性不足意味着,在低收入和中等收入国家(LMIC),医院在新冠病毒感染增加期间有不堪重负的风险。在疫情初期,高收入地区已制定了用于急诊科(ED)快速分诊入院需求的风险评分。
利用2020年8月27日至2022年3月11日南非西开普省公立医院的常规收集数据,得出一个包含446,084例疑似新冠病毒感染的急诊科患者队列。主要结局为30天时死亡或入住重症监护病房(ICU)。该队列被分为推导集和奥密克戎变异株验证集。我们根据推导队列中的多变量分析系数和现有的分诊方法制定了LMIC-PRIEST评分。我们在奥密克戎时期队列和一个英国队列中对其准确性进行了外部验证。
我们分析了305,564例病例,其中推导集140,520例,奥密克戎时期队列12,610例,英国验证队列12,610例。对每个预测参数建模的事件超过100个。多变量分析确定了八个在各模型中均保留的预测变量。我们利用这些结果和临床判断,基于南非分诊早期预警评分制定了一个评分,还纳入了年龄、性别、血氧饱和度、吸入氧、糖尿病和心脏病。LMIC-PRIEST评分的C统计量为:推导队列0.82(95%置信区间:0.82至0.83);奥密克戎时期队列0.79(95%置信区间:0.78至0.80);英国队列0.79(95%置信区间:0.79至0.80)。结局患病率的差异导致外部验证中的校准不完善。然而,在三分或更低的阈值使用该评分,将能够识别极低风险患者(阴性预测值≥0.99),这些患者可以根据初始评估收集的信息迅速出院。
LMIC-PRIEST评分在较低阈值下显示出良好的区分度和高灵敏度,可用于在LMIC急诊科环境中快速识别低风险患者。
低收入和中等收入国家(LMIC)疫苗接种不均衡,加上医疗保健供应韧性不足,意味着LMIC的紧急医疗保健系统在新冠病毒感染增加期间仍可能有不堪重负的风险。风险分层评分可能有助于快速分诊住院需求。然而,那些提议用于疑似新冠病毒感染患者急诊科的评分是在高收入地区制定和验证的。
LMIC-PRIEST评分是利用南非西开普省的一个大型常规数据集稳健地制定的,并且直接适用于LMIC现有的分诊方法。在不同收入环境和新冠病毒变异株中的外部验证表明,该评分对表明需要从急诊科住院的综合结局具有良好的区分度和高灵敏度(在较低阈值下)。
在三分或更低的阈值使用LMIC-PRIEST评分,将能够在所有评估环境中识别极低风险患者(阴性预测值≥0.99)。在需求增加期间,这可以利用初始评估收集的信息,快速识别急诊科患者并使其出院。