D'Amario Domenico, Ciliberti Giuseppe, Restivo Attilio, Laborante Renzo, Migliaro Stefano, Canonico Francesco, Sangiorgi Giuseppe Massimo, Tebaldi Matteo, Porto Italo, Andreini Daniele, Vergallo Rocco, Leone Antonio Maria, Gervasi Salvatore, Cammarano Michela, Palmieri Vincenzo, Burzotta Francesco, Trani Carlo, Zeppilli Paolo, Crea Filippo
Department of Cardiovascular and Thoracic Sciences, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome 00168, Italy.
Catholic University of the Sacred Heart, Rome 00168, Italy.
Eur Heart J Suppl. 2022 Nov 11;24(Suppl H):H48-H56. doi: 10.1093/eurheartjsupp/suac059. eCollection 2022 Nov.
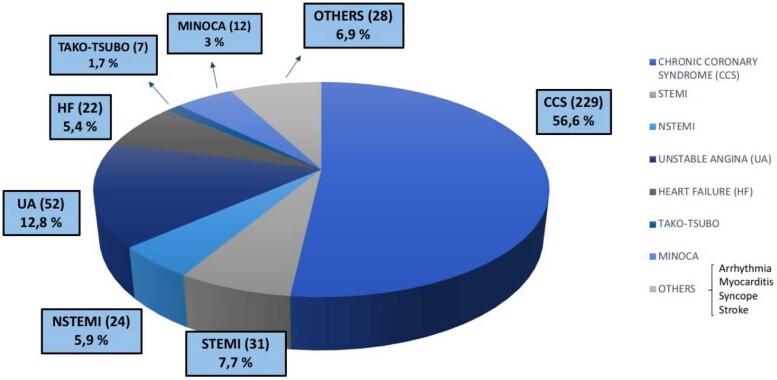
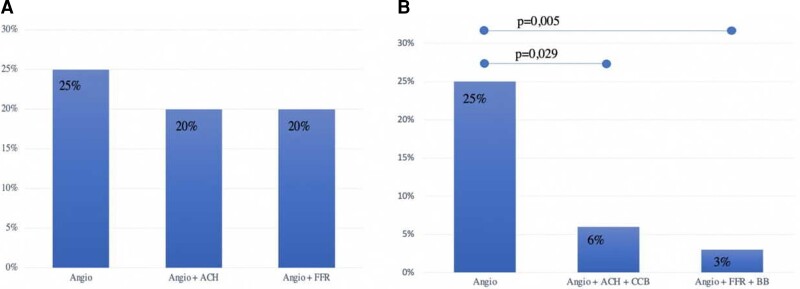
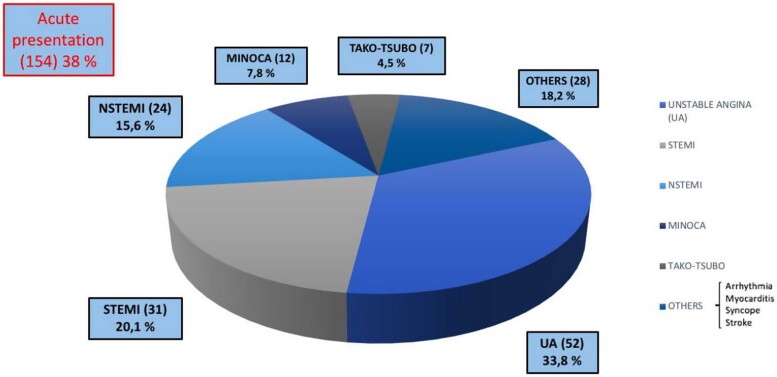
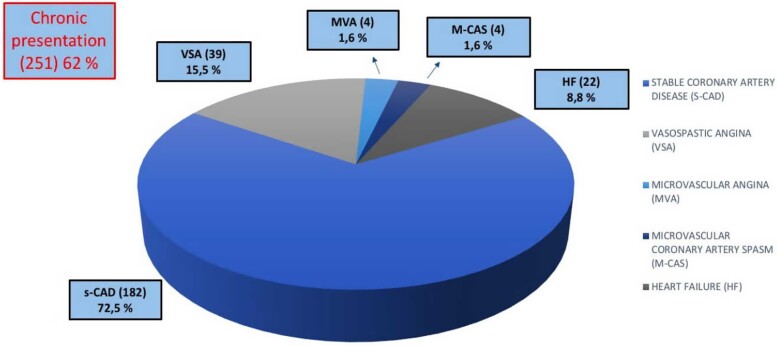
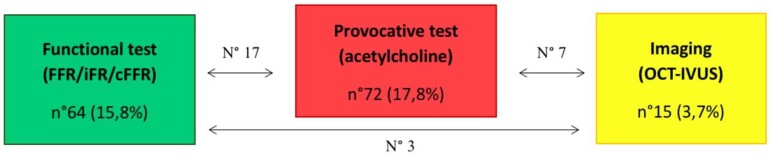
Myocardial bridge (MB) is the most frequent inborn coronary artery variant in which a portion of the myocardium overlies an epicardial coronary artery segment. Although MB has long been considered a benign entity, a growing body of evidence has suggested its association with angina and adverse cardiac events. However, to date, no data on long-term prognosis are available, nor on therapies improving cardiovascular outcomes. We are currently conducting an ambispective, observational, multicentre, study in which we enrol patients with a clinical indication to undergo coronary angiography (CA) and evidence of MB, aiming to describe the incidence of symptoms and cardiovascular events at baseline and at long-term follow-up (FUP). The role of invasive full-physiology assessment in modifying the discharge therapy and eventually the perceived quality of life and the incidence of major cardiovascular events will be analysed. Basal clinical-instrumental data of eligible and consenting patients have been acquired after CA; FUP was performed 6, 12, and 24 months after the angiographic diagnosis of MB. The primary endpoint of the study is the incidence of major adverse cardiovascular events (MACE), defined as the composite of cardiac death, myocardial infarction, cardiac hospitalization, and target vessel revascularization; the secondary endpoints are the rate of patients with Seattle Angina Questionnaire (SAQ) summary score <70 and the incidence of MACE in patients undergoing invasive intracoronary assessment. Among patients undergone FUP visits, we recorded 31 MACE at 6 months (11.6%), 16 MACE at 12 months (6.5%), and 26 MACE at 24 months (13.5%). The rate of patients with SAQ <70 is 18.8% at 6 months, 20.6% at 12 months, and 21.8% at 24 months. To evaluate the prognostic role of invasive intracoronary assessment, we compared MB patients who underwent only angiographic evaluation (Angio group) to those who underwent acetylcholine (ACH) provocative test with indication to calcium-channel blockers (CCBs) at discharge (Angio + ACH + CCBs group) and those who underwent functional assessment with fractional flow reserve (FFR) with indication to beta-blockers (BBs) at discharge (Angio + FFR + BBs group). After 2 years of FUP, the rate of MACE was significantly reduced in both Angio + ACH + CCBs group (6 vs. 25%, = 0.029) and Angio + FFR + BBs group (3 vs. 25%, = 0.005) compared with Angio group. The preliminary results of our study showed that MB may be a cause of angina and adverse cardiac events in patients referred to CA for suspected coronary artery disease (CAD). Full-physiology assessment unmasking MB-related ischaemia mechanisms, allowed to guide the treatment, personalizing the clinical management, improving the quality of life, and cardiovascular outcomes in patients with MB.
心肌桥(MB)是最常见的先天性冠状动脉变异,即一部分心肌覆盖于心外膜冠状动脉节段之上。尽管长期以来MB一直被认为是一种良性病变,但越来越多的证据表明它与心绞痛及不良心脏事件有关。然而,迄今为止,尚无关于长期预后的数据,也没有关于改善心血管结局的治疗方法的数据。我们目前正在进行一项双向、观察性、多中心研究,纳入有临床指征接受冠状动脉造影(CA)且有MB证据的患者,旨在描述基线及长期随访(FUP)时症状和心血管事件的发生率。将分析有创全生理学评估在改变出院治疗方案、最终改善生活质量和降低主要心血管事件发生率方面的作用。在CA后已获取符合条件并同意参与研究的患者的基础临床检查数据;在MB血管造影诊断后的6、12和24个月进行FUP。该研究的主要终点是主要不良心血管事件(MACE)的发生率,MACE定义为心脏死亡、心肌梗死、心脏住院和靶血管血运重建的综合情况;次要终点是西雅图心绞痛问卷(SAQ)总分<70分的患者比例以及接受有创冠状动脉内评估的患者中MACE的发生率。在接受FUP随访的患者中,我们记录到6个月时发生31例MACE(11.6%),12个月时发生16例MACE(6.5%),24个月时发生26例MACE(13.5%)。SAQ<70分的患者比例在6个月时为18.8%,12个月时为20.6%,24个月时为21.8%。为评估有创冠状动脉内评估的预后作用,我们将仅接受血管造影评估的MB患者(血管造影组)与那些接受乙酰胆碱(ACH)激发试验且出院时给予钙通道阻滞剂(CCB)治疗的患者(血管造影+ACH+CCB组)以及那些接受血流储备分数(FFR)功能评估且出院时给予β受体阻滞剂(BB)治疗的患者(血管造影+FFR+BB组)进行了比较。FUP 2年后,与血管造影组相比,血管造影+ACH+CCB组(6%对25%,P = 0.029)和血管造影+FFR+BB组(3%对25%,P = 0.005)的MACE发生率均显著降低。我们研究的初步结果表明,对于因疑似冠状动脉疾病(CAD)而接受CA检查的患者,MB可能是心绞痛和不良心脏事件的一个原因。揭示与MB相关的缺血机制的全生理学评估能够指导治疗,使临床管理个体化,改善MB患者的生活质量和心血管结局。