Department of Cardiovascular Medicine Fondazione Policlinico Universitario A. Gemelli IRCCS Rome Italy.
Department of Cardiovascular and Pulmonary Sciences Catholic University of the Sacred Heart Rome Italy.
J Am Heart Assoc. 2021 Jul 20;10(14):e020535. doi: 10.1161/JAHA.120.020535. Epub 2021 Jul 14.
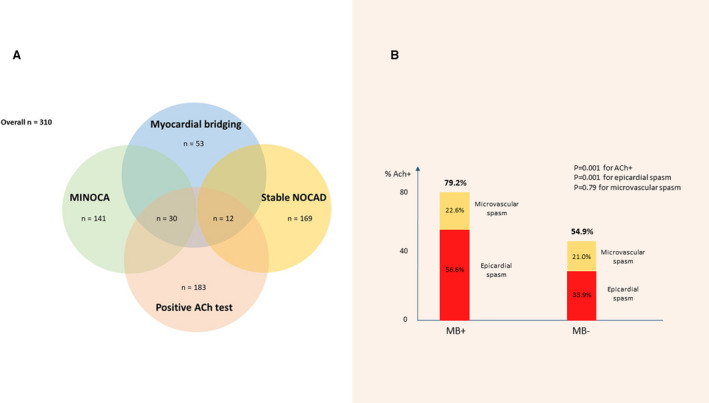
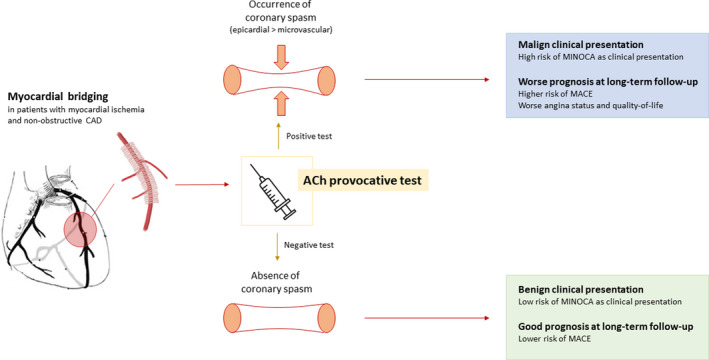
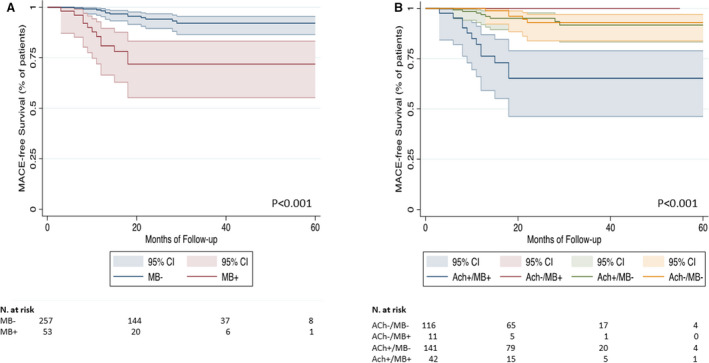
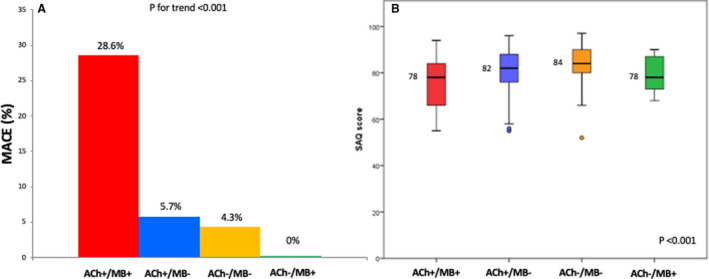
Background Myocardial bridging (MB) may represent a cause of myocardial ischemia in patients with non-obstructive coronary artery disease (NOCAD). Herein, we assessed the interplay between MB and coronary vasomotor disorders, also evaluating their prognostic relevance in patients with myocardial infarction and non-obstructive coronary arteries (MINOCA) or stable NOCAD. Methods and Results We prospectively enrolled patients with NOCAD undergoing intracoronary acetylcholine provocative test. The incidence of major adverse cardiac events, defined as the composite of cardiac death, non-fatal myocardial infarction, and rehospitalization for unstable angina, was assessed at follow-up. We also assessed angina status using Seattle Angina Questionnaires summary score. We enrolled 310 patients (mean age, 60.6±11.9; 136 [43.9%] men; 169 [54.5%] stable NOCAD and 141 [45.5%] MINOCA). MB was found in 53 (17.1%) patients. MB and a positive acetylcholine test coexisted more frequently in patients with MINOCA versus stable NOCAD. MB was an independent predictor of positive acetylcholine test and MINOCA. At follow-up (median, 22 months; interquartile range, 13-32), patients with MB had a higher rate of major adverse cardiac events, mainly driven by a higher rate of hospitalization attributable to angina, and a lower Seattle Angina Questionnaires summary score (all <0.001) compared with patients without MB. In particular, the group of patients with MB and a positive acetylcholine test had the worst prognosis. Conclusions Among patients with NOCAD, coronary spasm associated with MB may predict a worse clinical presentation with MINOCA and a higher rate of hospitalization attributable to angina at long-term follow-up with a low rate of hard events.
心肌桥(MB)可能是无阻塞性冠状动脉疾病(NOCAD)患者心肌缺血的原因。在此,我们评估了 MB 与冠状动脉舒缩功能障碍之间的相互作用,并评估了它们在心肌梗死伴非阻塞性冠状动脉(MINOCA)或稳定 NOCAD 患者中的预后相关性。
我们前瞻性纳入了接受冠状动脉乙酰胆碱激发试验的 NOCAD 患者。在随访时评估主要不良心脏事件(定义为心脏死亡、非致死性心肌梗死和不稳定型心绞痛再住院的复合终点)的发生率。我们还使用西雅图心绞痛问卷综合评分评估心绞痛情况。我们纳入了 310 名患者(平均年龄 60.6±11.9 岁;136 [43.9%] 名男性;169 [54.5%] 名稳定 NOCAD 和 141 [45.5%] MINOCA)。53 名(17.1%)患者存在 MB。MB 和阳性乙酰胆碱试验在 MINOCA 患者中比在稳定 NOCAD 患者中更常见。MB 是阳性乙酰胆碱试验和 MINOCA 的独立预测因子。在随访期间(中位数 22 个月;四分位距 13-32),与无 MB 的患者相比,有 MB 的患者主要因心绞痛住院的比例更高,且西雅图心绞痛问卷综合评分更低,其主要不良心脏事件发生率更高(均<0.001)。特别是,MB 合并阳性乙酰胆碱试验的患者组预后最差。
在 NOCAD 患者中,与 MB 相关的冠状动脉痉挛可能预示着 MINOCA 患者的临床表现更差,且在长期随访中因心绞痛导致住院的比例更高,硬终点事件发生率较低。