Dementia Research Centre, Department of Neurodegenerative Disease, UCL Queen Square Institute of Neurology, Queen Square, London, WC1N 3BG, UK.
Department of Medical Statistics, London School of Hygiene and Tropical Medicine, London, UK.
J Neurol. 2023 Mar;270(3):1466-1477. doi: 10.1007/s00415-022-11442-y. Epub 2022 Nov 17.
To investigate the optimal method of adding motor features to a clinical rating scale for frontotemporal dementia (FTD).
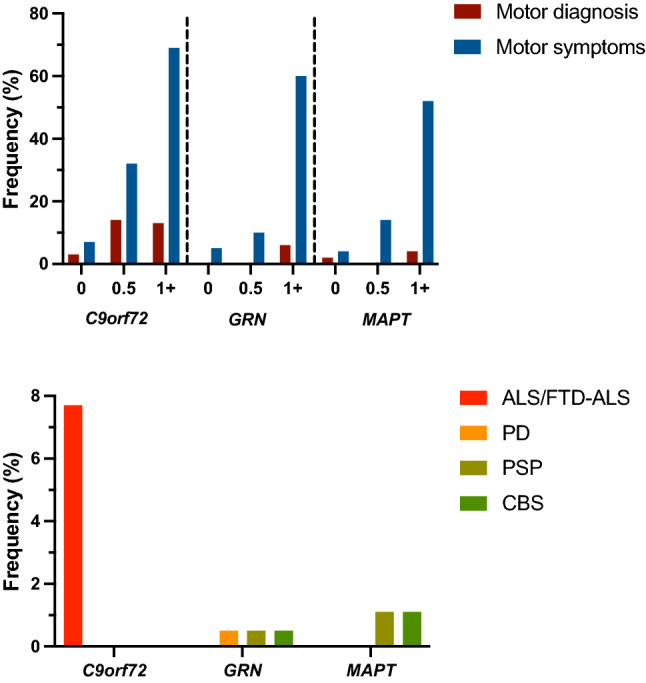
Eight hundred and thirty-two participants from the international multicentre Genetic FTD Initiative (GENFI) study were recruited: 522 mutation carriers (with C9orf72, GRN and MAPT mutations) and 310 mutation-negative controls. A standardised clinical questionnaire was used to assess eight motor symptoms (dysarthria, dysphagia, tremor, slowness, weakness, gait disorder, falls and functional difficulties using hands). Frequency and severity of each motor symptom was assessed, and a principal component analysis (PCA) was performed to identify how the different motor symptoms loaded together. Finally, addition of a motor component to the CDR plus NACC FTLD was investigated (CDR plus NACC FTLD-M).
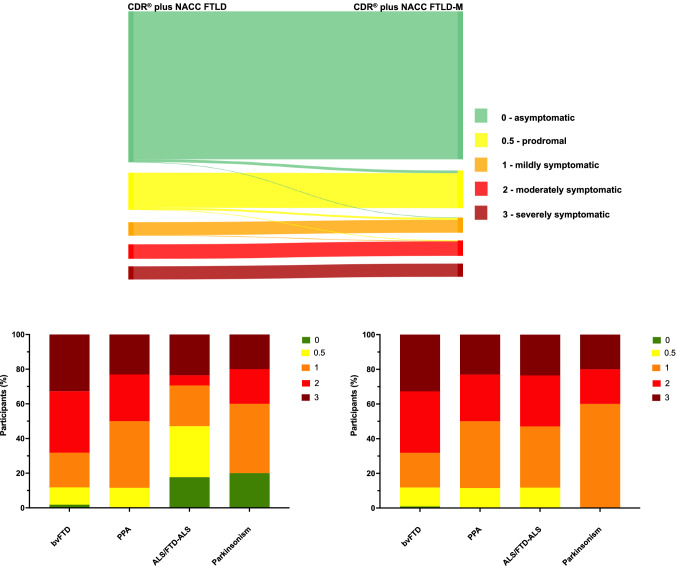
24.3% of mutation carriers had motor symptoms (31.7% C9orf72, 18.8% GRN, 19.3% MAPT) compared to 6.8% of controls. Slowness and gait disorder were the commonest in all genetic groups while tremor and falls were the least frequent. Symptom severity scores were similar to equivalent physical motor examination scores. PCA revealed that all motor symptoms loaded together so a single additional motor component was added to the CDR plus NACC FTLD to form the CDR plus NACC FTLD-M. Individual global scores were more severe with the CDR plus NACC FTLD-M, and no patients with a clinically diagnosed motor disorder (ALS/FTD-ALS or parkinsonism) were classified anymore as asymptomatic (unlike the CDR plus NACC FTLD alone).
Motor features are present in mutation carriers at all disease stages across all three genetic groups. Inclusion of motor symptoms in a rating scale that can be used in future clinical trials will not only ensure a more accurate severity measure is recorded but that a wider spectrum of FTD phenotypes can be included in the same trial.
探索为额颞叶痴呆(FTD)临床评分量表添加运动特征的最佳方法。
国际多中心遗传 FTD 倡议(GENFI)研究共招募了 832 名参与者:522 名突变携带者(携带 C9orf72、GRN 和 MAPT 突变)和 310 名突变阴性对照者。采用标准化临床问卷评估八项运动症状(构音障碍、吞咽困难、震颤、运动缓慢、无力、步态障碍、跌倒和手部功能障碍)。评估每种运动症状的频率和严重程度,并进行主成分分析(PCA)以确定不同运动症状如何共同加载。最后,研究了将运动成分添加到 CDR 加 NACC FTLD 中的情况(CDR 加 NACC FTLD-M)。
与对照组的 6.8%相比,突变携带者中有 24.3%(31.7%为 C9orf72,18.8%为 GRN,19.3%为 MAPT)出现运动症状。在所有遗传组中,运动缓慢和步态障碍最为常见,而震颤和跌倒则最为罕见。症状严重程度评分与等效的物理运动检查评分相似。PCA 显示所有运动症状均共同加载,因此在 CDR 加 NACC FTLD 中添加了一个单一的额外运动成分,形成了 CDR 加 NACC FTLD-M。使用 CDR 加 NACC FTLD-M,个体总体评分更为严重,并且不再将具有临床诊断的运动障碍(ALS/FTD-ALS 或帕金森病)的患者归类为无症状(与单独使用 CDR 加 NACC FTLD 不同)。
在所有三种遗传组中,在疾病的各个阶段,突变携带者均存在运动特征。在可以用于未来临床试验的评分量表中纳入运动症状,不仅可以确保更准确地记录严重程度,而且可以在同一试验中纳入更广泛的 FTD 表型。