Department of Pathology-Medical Microbiology, Faculty of Medicine, University of Medical Sciences and Technology, Khartoum, Sudan.
Department of Clinical Microbiology, Umeå University, Umeå, Sweden.
Medicine (Baltimore). 2022 Nov 18;101(46):e31588. doi: 10.1097/MD.0000000000031588.
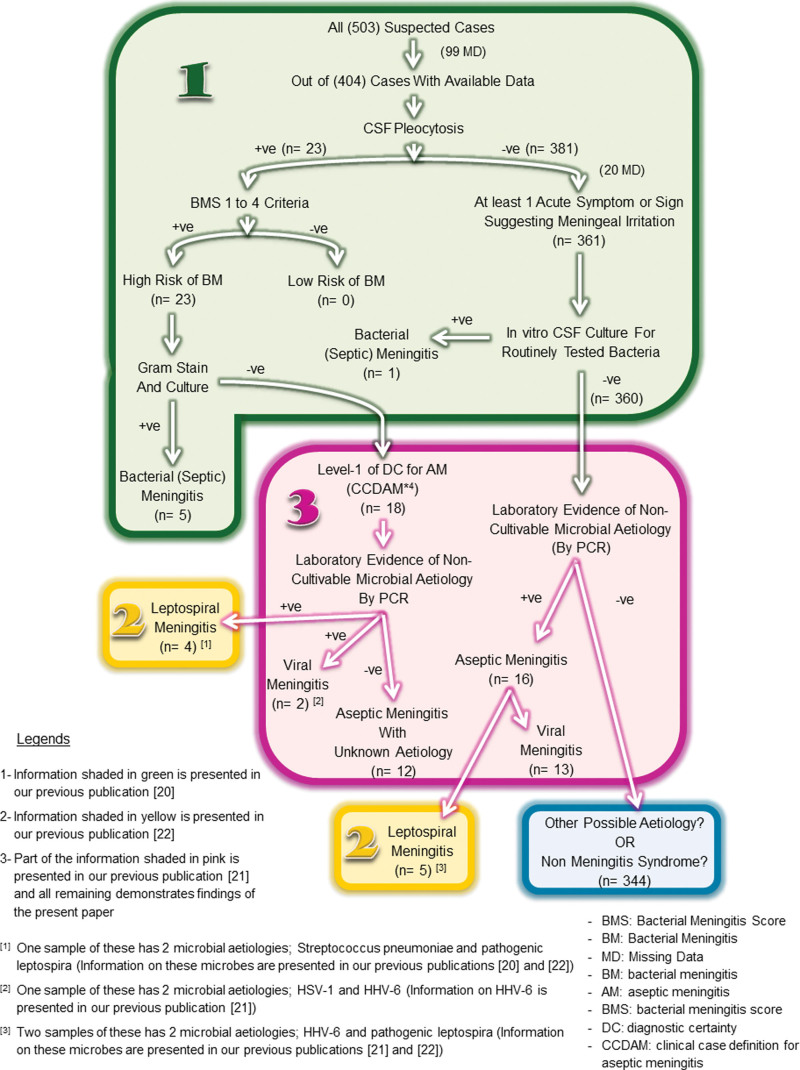
Diagnosis of viral meningitis (VM) is uncommon practice in Sudan and there is no local viral etiological map. We therefore intended to differentiate VM using standardized clinical codes and determine the involvement of herpes simplex virus types-1 and 2 (HSV-1/2), varicella zoster virus, non-polio human enteroviruses (HEVs), and human parechoviruses in meningeal infections in children in Sudan. This is a cross-sectional hospital-based study. Viral meningitis was differentiated in 503 suspected febrile attendee of Omdurman Hospital for Children following the criteria listed in the Clinical Case Definition for Aseptic/Viral Meningitis. Patients were children age 0 to 15 years. Viral nucleic acids (DNA/RNA) were extracted from cerebrospinal fluid (CSF) specimens using QIAamp® UltraSens Virus Technology. Complementary DNA was prepared from viral RNA using GoScriptTM Reverse Transcription System. Viral nucleic acids were amplified and detected using quantitative TaqMan® Real-Time and conventional polymerase chain reactions (PCRs). Hospital diagnosis of VM was assigned to 0%, when clinical codes were applied; we considered 3.2% as having VM among the total study population and as 40% among those with proven infectious meningitis. Two (0.4%) out of total 503 CSF specimens were positive for HSV-1; Ct values were 37.05 and 39.10 and virus copies were 652/PCR run (261 × 103/mL CSF) and 123/PCR run (49.3 × 103/mL CSF), respectively. Other 2 (0.4%) CSF specimens were positive for non-polio HEVs; Ct values were 37.70 and 38.30, and the approximate virus copies were 5E2/PCR run (2E5/mL CSF) and 2E2/PCR run (8E4/mL CSF), respectively. No genetic materials were detected for HSV-2, varicella zoster virus, and human parechoviruses. The diagnosis of VM was never assigned by the hospital despite fulfilling the clinical case definition. Virus detection rate was 10% among cases with proven infectious meningitis. Detected viruses were HSV-1 and non-polio HEVs. Positive virus PCRs in CSFs with normal cellular counts were seen.
在苏丹,病毒性脑膜炎(VM)的诊断并不常见,也没有本地的病毒病因图谱。因此,我们旨在使用标准化的临床代码来区分 VM,并确定单纯疱疹病毒 1 型和 2 型(HSV-1/2)、水痘带状疱疹病毒、非脊髓灰质炎人类肠道病毒(HEVs)和人类肠道病毒在苏丹儿童脑膜感染中的作用。这是一项基于医院的横断面研究。根据无菌/病毒性脑膜炎临床病例定义中列出的标准,对奥姆杜尔曼儿童医院的 503 名疑似发热就诊者进行病毒性脑膜炎鉴别诊断。患者为 0 至 15 岁的儿童。使用 QIAamp®UltraSens Virus 技术从脑脊液(CSF)标本中提取病毒核酸(DNA/RNA)。使用 GoScriptTM Reverse Transcription System 从病毒 RNA 制备互补 DNA。使用定量 TaqMan®实时和常规聚合酶链反应(PCR)扩增和检测病毒核酸。当应用临床代码时,医院诊断为 VM 的比例为 0%;我们认为在总研究人群中,有 3.2%患有 VM,在有明确感染性脑膜炎的人群中,有 40%患有 VM。503 份 CSF 标本中,有 2 份(0.4%)为 HSV-1 阳性;Ct 值分别为 37.05 和 39.10,病毒拷贝数分别为 652/PCR 运行(261×103/ml CSF)和 123/PCR 运行(49.3×103/ml CSF)。另外 2 份(0.4%)CSF 标本为非脊髓灰质炎 HEVs 阳性;Ct 值分别为 37.70 和 38.30,近似病毒拷贝数分别为 5E2/PCR 运行(2E5/ml CSF)和 2E2/PCR 运行(8E4/ml CSF)。未检测到 HSV-2、水痘带状疱疹病毒和人类肠道病毒的遗传物质。尽管符合临床病例定义,但医院从未诊断过 VM。在有明确感染性脑膜炎的病例中,病毒检出率为 10%。检测到的病毒为 HSV-1 和非脊髓灰质炎 HEVs。在细胞计数正常的 CSF 中也可见到阳性病毒 PCR。