Department of Anesthesiology, Affiliated Hospital of North Sichuan Medical College, No.1 Maoyuan South Road, Nanchong, 637000, Sichuan, China.
Department of Anesthesiology, Zigong First People's Hospital, Zigong, Sichuan, China.
BMC Geriatr. 2022 Nov 19;22(1):882. doi: 10.1186/s12877-022-03619-x.
Postinduction hypotension is closely related to postoperative complications. Elderly patients with compromised cardiovascular compensatory reserve are more susceptible to hypotension after induction of general anesthesia. This study investigated whether the carotid artery corrected flow time (FTc) and respiratory variation of peak blood flow velocity in the common carotid artery (ΔVpeak) could predict postinduction hypotension in elderly patients.
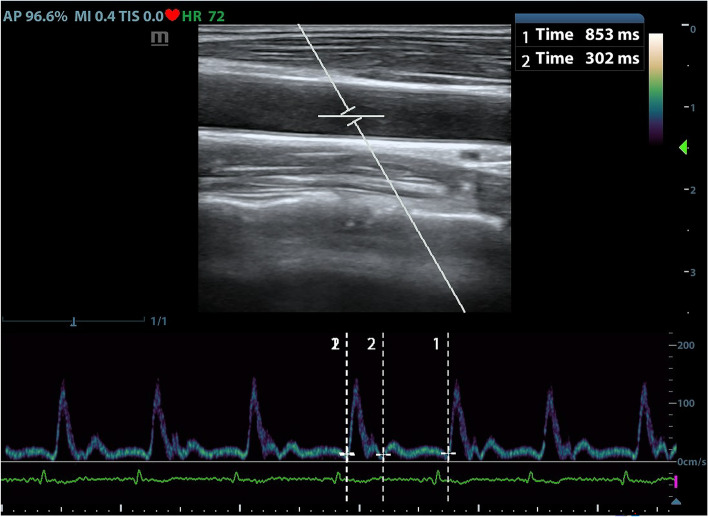
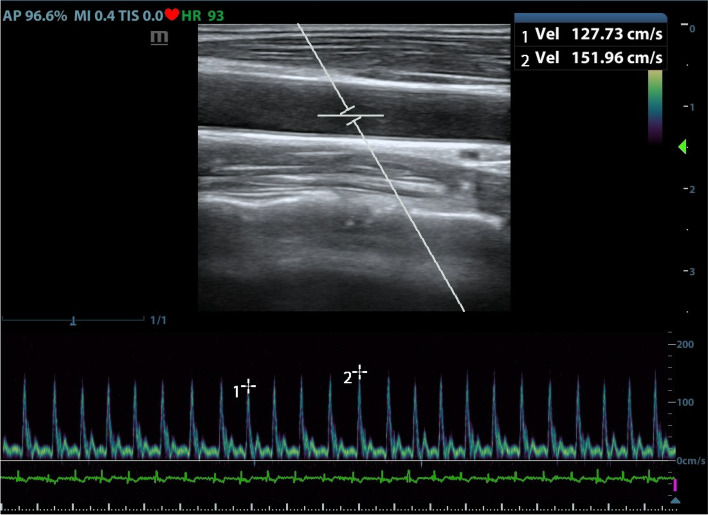
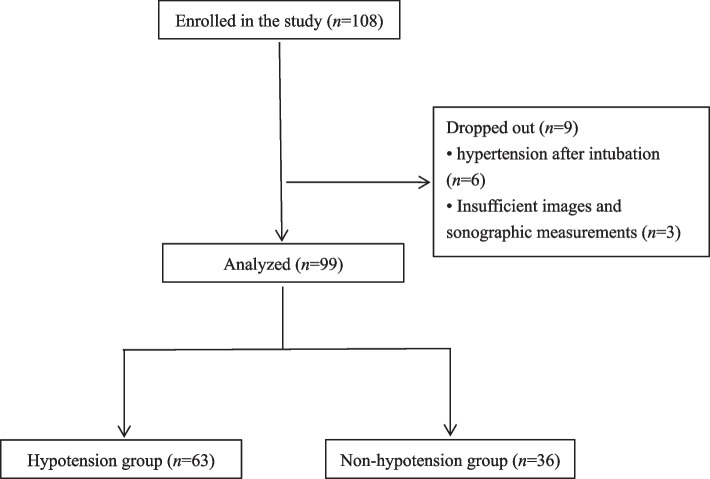
This prospective observational study included elderly patients aged 65 to 75 who were scheduled for elective surgery under general anesthesia with ASA physical status class of I-II, without cardiovascular disease, hypertension, diabetes, or obesity. Anesthesia was induced by midazolam, sufentanil, and etomidate and was maintained by sevoflurane. The carotid artery FTc and ΔVpeak were measured by ultrasound before induction of anesthesia. Hemodynamic data were recorded before induction and then during the first 10 min after induction.
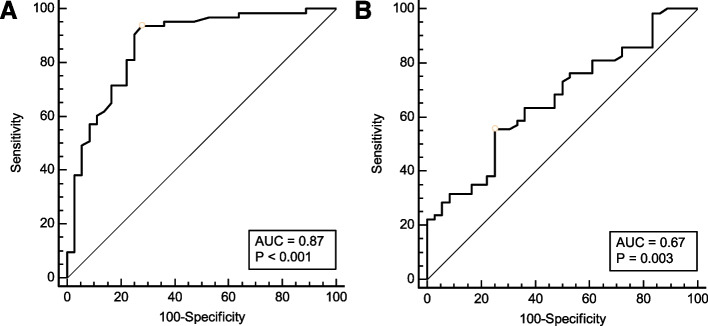
Ninety-nine patients were included in the final analysis, of whom 63 developed postinduction hypotension. The area under the receiver operating characteristic curves was 0.87 (0.78 to 0.93) for carotid artery FTc and 0.67 (0.56 to 0.76) for ΔVpeak, respectively. The optimal cutoff value for predicting postinduction hypotension was 379.1 ms for carotid artery FTc, with sensitivity and specificity of 72.2 and 93.7%, respectively. The best cutoff value was 7.5% for ΔVpeak, with sensitivity and specificity of 55.6 and 75.0%, respectively.
The carotid artery FTc is a reliable predictor of postinduction hypotension in elderly patients with ASA status of I or II, without cardiovascular disease, hypertension, diabetes, or obesity. Elderly patients with a carotid artery FTc less than 379.1 ms before anesthesia have a higher risk of postinduction hypotension.
Clinical Trial Registry on August 2nd, 2020 ( www.chictr.org.cn ; ChiCTR2000035190).
诱导后低血压与术后并发症密切相关。心血管代偿储备能力受损的老年患者在全身麻醉诱导后更容易发生低血压。本研究旨在探讨颈动脉校正流量时间(FTc)和颈总动脉血流速度峰值呼吸变异度(ΔVpeak)是否可预测老年患者全麻诱导后低血压。
本前瞻性观察研究纳入了 99 例年龄 65 至 75 岁、ASA 身体状况 I-II 级、无心血管疾病、高血压、糖尿病或肥胖的择期全麻手术患者。麻醉诱导采用咪达唑仑、舒芬太尼和依托咪酯,七氟醚维持麻醉。麻醉诱导前通过超声测量颈动脉 FTc 和 ΔVpeak。记录麻醉诱导前和诱导后 10 分钟内的血流动力学数据。
最终分析纳入 99 例患者,其中 63 例发生诱导后低血压。颈动脉 FTc 和 ΔVpeak 预测诱导后低血压的受试者工作特征曲线下面积分别为 0.87(0.78 至 0.93)和 0.67(0.56 至 0.76)。颈动脉 FTc 预测诱导后低血压的最佳截断值为 379.1ms,灵敏度和特异度分别为 72.2%和 93.7%。ΔVpeak 的最佳截断值为 7.5%,灵敏度和特异度分别为 55.6%和 75.0%。
对于 ASA 分级 I 或 II、无心血管疾病、高血压、糖尿病或肥胖的老年患者,颈动脉 FTc 是预测全麻诱导后低血压的可靠指标。麻醉前颈动脉 FTc 小于 379.1ms 的老年患者发生全麻诱导后低血压的风险较高。
2020 年 8 月 2 日在中国临床试验注册中心( www.chictr.org.cn ; ChiCTR2000035190)注册。