Southern California Permanente Medical Group, Neurology Department, Kaiser Permanente Southern California, Los Angeles, USA; Department of Clinical Science, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, USA.
Department of Research and Evaluation, Kaiser Permanente Southern California, Pasadena, USA.
Int J Infect Dis. 2022 Dec;125:184-191. doi: 10.1016/j.ijid.2022.10.023. Epub 2022 Oct 29.
To assess whether high- compared with low-dose corticosteroids started upon hospitalization reduce mortality in patients with severe COVID-19 pneumonia or in subgroups stratified by severity of respiratory impairment on admission.
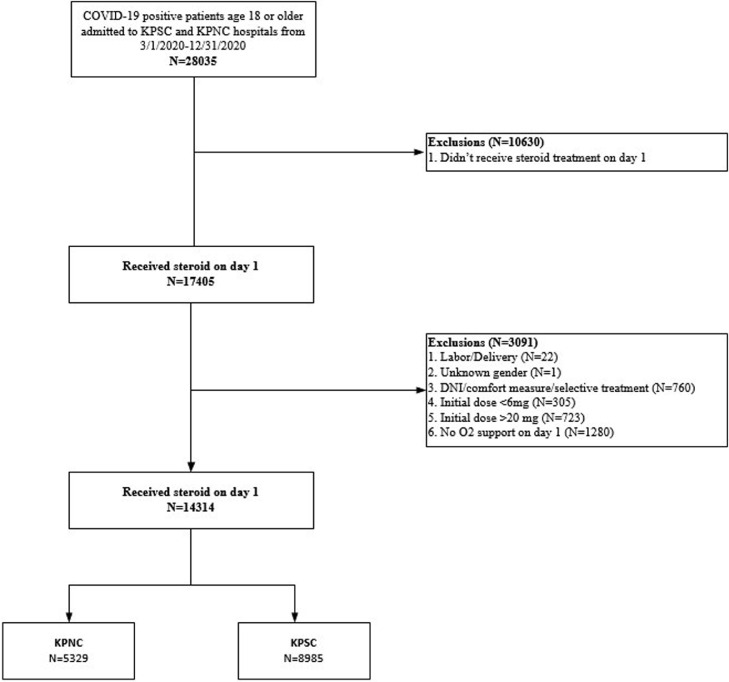
We conducted a retrospective cohort study of patients with confirmed SARS-CoV-2 infection who required oxygen supplementation upon hospitalization between March 1 and December 31, 2020. In-hospital death was analyzed using logistic regression with inverse probability of treatment weighting of receiving low- or high-dose corticosteroid (dexamethasone 6-10 mg daily or >10-20 mg daily or other corticosteroid equivalents).
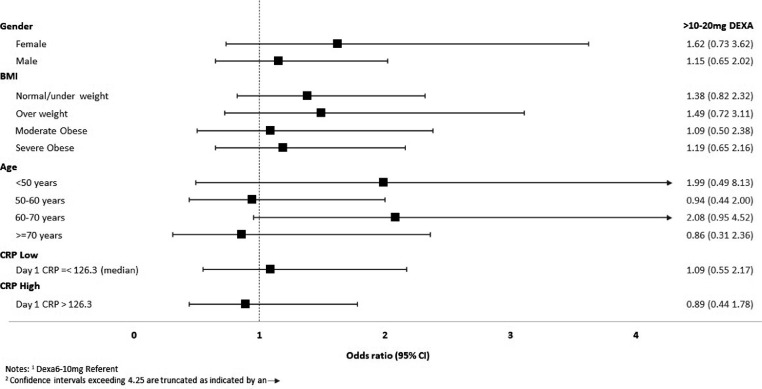
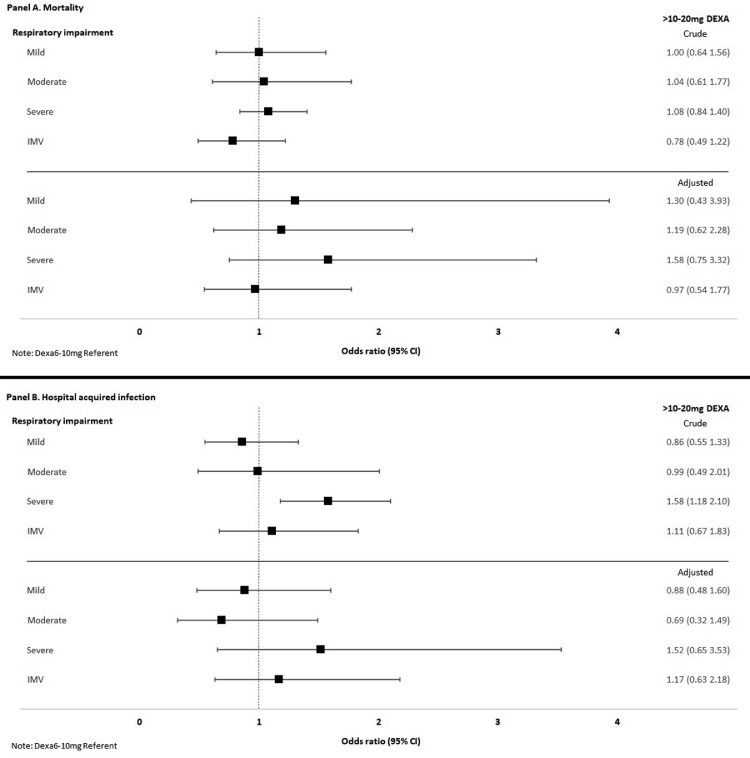
We analyzed 13,366 patients who received low-dose and 948 who received high-dose corticosteroids, of whom 31.3% and 40.4% had severe respiratory impairment (>15 l/min of oxygen or mechanical ventilation) upon admission, respectively. There were no differences in the propensity score-adjusted odds of death (odds ratio 1.17, 95% CI 0.72-1.90) or infections (odds ratio 0.70, 95% CI 0.44-1.11) for patients who received high-dose compared with low-dose corticosteroids, beginning on the day of admission. No significant differences in subgroups stratified by severity of respiratory impairment were found.
Initiating high-dose compared with low-dose corticosteroids among newly hospitalized patients with COVID-19 pneumonia did not improve survival. However, benefit of high-dose corticosteroids in specific subgroups cannot be excluded.
评估入院时使用高剂量与低剂量皮质类固醇治疗是否能降低重症 COVID-19 肺炎患者或按入院时呼吸功能损害严重程度分层的亚组患者的死亡率。
我们对 2020 年 3 月 1 日至 12 月 31 日期间因需要住院补充氧气而确诊 SARS-CoV-2 感染的患者进行了回顾性队列研究。使用逻辑回归分析入院时接受低剂量或高剂量皮质类固醇(地塞米松 6-10 mg/天或>10-20 mg/天或其他皮质类固醇等效物)治疗的患者的院内死亡率,并对其进行逆概率治疗加权处理。
我们分析了 13366 例接受低剂量皮质类固醇治疗的患者和 948 例接受高剂量皮质类固醇治疗的患者,其中分别有 31.3%和 40.4%的患者入院时呼吸功能损害严重(>15 l/min 的氧气或机械通气)。与低剂量皮质类固醇相比,高剂量皮质类固醇在入院当天开始治疗的患者中,其死亡率(比值比 1.17,95%置信区间 0.72-1.90)或感染率(比值比 0.70,95%置信区间 0.44-1.11)无差异。在按呼吸功能损害严重程度分层的亚组中,也未发现显著差异。
与 COVID-19 肺炎新入院患者相比,起始高剂量皮质类固醇治疗并不能提高生存率。然而,也不能排除高剂量皮质类固醇在特定亚组中的获益。