Department of Research & Evaluation, Southern California Permanente Medical Group, Pasadena.
Department of Neurology, Los Angeles Medical Center, Southern California Permanente Medical Group, Los Angeles.
JAMA Netw Open. 2022 Dec 1;5(12):e2248664. doi: 10.1001/jamanetworkopen.2022.48664.
Rituximab and other B-cell-depleting therapies blunt humoral responses to SARS-CoV-2 vaccines, particularly when the vaccine is administered within 6 months of an infusion. Whether this translates into an increased risk of hospitalization or death from COVID-19 is unclear.
To examine whether rituximab treatment is associated with an increased risk of hospitalization for COVID-19 among SARS-CoV-2-vaccinated persons with multiple sclerosis (MS) and whether delaying vaccination more than 6 months after rituximab treatment is associated with decreased risk.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used Kaiser Permanente Southern California's electronic health record to identify individuals from January 1, 2020, to February 15, 2022, who had MS and who had been vaccinated against SARS-CoV-2.
Rituximab treatment compared with disease-modifying therapies (DMTs) that do not interfere with vaccine efficacy or being untreated (no or other DMT group). Among rituximab-treated patients, the exposure was receiving at least 1 vaccine dose more than 6 months after their last infusion compared with receiving all vaccine doses 6 months or less since their last infusion.
The main outcome was hospitalization due to COVID-19 infection. The odds of infection resulting in hospitalization following SARS-CoV-2 vaccination were adjusted for race and ethnicity, advanced MS-related disability; vaccine type; booster dose; and, among rituximab-treated only analyses, cumulative rituximab dose and dose at last infusion. Exposures, outcomes, and covariates were collected from the electronic health record.
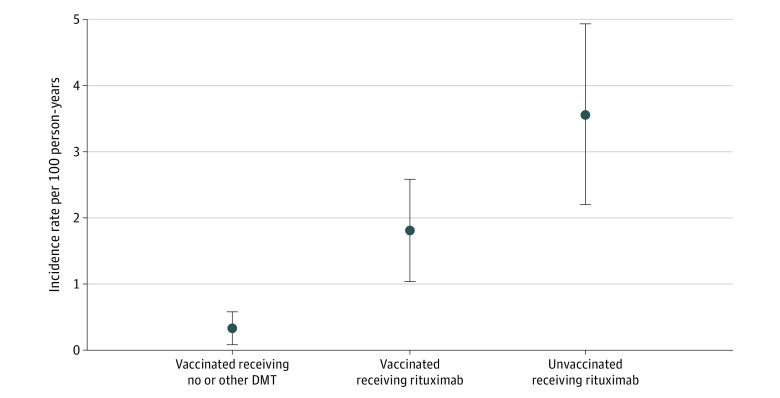
Among 3974 SARS-CoV-2-vaccinated people with MS (mean [SD] age, 55.3 [15] years; 2982 [75.0%] female; 103 [2.6%] Asian or Pacific Islander; 634 [16.0%] Black; 953 [24.0%] Hispanic; 2269 [57.1%] White; and 15 [0.3%] other race or ethnicity), rituximab-treated patients (n = 1516) were more likely to be hospitalized (n = 27) but not die (n = 0) compared with the 2458 individuals with MS receiving no or other DMTs (n = 7 and n = 0, respectively; adjusted odds ratio [aOR] for hospitalization, 7.33; 95% CI, 3.05-17.63). Receiving messenger RNA (mRNA) SARS-CoV-2 vaccine (aOR, 0.36; 95% CI, 0.15-0.90; P = .03) and receiving a booster vaccination (aOR, 0.31; 95% CI, 0.15-0.64; P = .002) were independently associated with a decreased risk of hospitalization for COVID-19. Among vaccinated rituximab-treated individuals with MS, receiving any vaccination dose more than 6 months after the last rituximab infusion was associated with a reduced risk of COVID-19 hospitalization (aOR, 0.22; 95% CI, 0.10-0.49).
This cohort study's findings suggest that rituximab-treated people with MS should be strongly encouraged to receive mRNA SARS-CoV-2 vaccines and boosters more than 6 months after their last rituximab infusion whenever possible. The low absolute risk of hospitalization for COVID-19 among mRNA-vaccinated individuals with MS should not preclude use of rituximab, which has marked efficacy, cost, and convenience advantages over other DMTs.
重要性:利妥昔单抗和其他 B 细胞耗竭疗法会削弱对 SARS-CoV-2 疫苗的体液免疫反应,尤其是当疫苗在输注后 6 个月内给予时。这是否会导致 COVID-19 住院或死亡的风险增加尚不清楚。
目的:检查利妥昔单抗治疗是否与多发性硬化症(MS)患者接受 SARS-CoV-2 疫苗接种后 COVID-19 住院风险增加相关,以及利妥昔单抗治疗后超过 6 个月延迟接种疫苗是否与风险降低相关。
设计、地点和参与者:这项回顾性队列研究使用 Kaiser Permanente Southern California 的电子健康记录,从 2020 年 1 月 1 日至 2022 年 2 月 15 日,确定了患有 MS 且已接种 SARS-CoV-2 疫苗的个体。
暴露:与不干扰疫苗效力或未接受治疗的疾病修正疗法(DMT)相比,利妥昔单抗治疗。在利妥昔单抗治疗的患者中,暴露是在最后一次输注后至少 6 个月接受至少 1 剂疫苗,而不是在最后一次输注后 6 个月内接受所有疫苗剂量。
主要结果和措施:主要结果是 COVID-19 感染导致的住院治疗。SARS-CoV-2 疫苗接种后感染导致住院的可能性在调整了种族和族裔、晚期 MS 相关残疾、疫苗类型、加强剂量以及仅在利妥昔单抗治疗的分析中,调整了累积利妥昔单抗剂量和最后一次输注剂量后,进行了调整。暴露、结局和协变量均从电子健康记录中收集。
结果:在 3974 名接受 SARS-CoV-2 疫苗接种的 MS 患者中(平均[SD]年龄,55.3[15]岁;2982 名[75.0%]女性;103 名[2.6%]亚洲或太平洋岛民;634 名[16.0%]黑人;953 名[24.0%]西班牙裔;2269 名[57.1%]白人;和 15 名[0.3%]其他种族或族裔),接受利妥昔单抗治疗的患者(n=1516)更有可能住院(n=27),但没有死亡(n=0),而接受无或其他 DMT 的 MS 患者(n=2458)分别为 7 人和 0 人(分别为调整后的比值比[OR],7.33;95%CI,3.05-17.63)。接受信使 RNA(mRNA)SARS-CoV-2 疫苗(调整后的 OR,0.36;95%CI,0.15-0.90;P=0.03)和接受加强疫苗接种(调整后的 OR,0.31;95%CI,0.15-0.64;P=0.002)与 COVID-19 住院风险降低独立相关。在接受利妥昔单抗治疗的 MS 患者中,在最后一次利妥昔单抗输注后 6 个月以上接受任何疫苗剂量与 COVID-19 住院风险降低相关(调整后的 OR,0.22;95%CI,0.10-0.49)。
结论和相关性:这项队列研究的结果表明,应强烈鼓励 MS 患者接受 mRNA SARS-CoV-2 疫苗和加强剂,只要有可能,就在最后一次利妥昔单抗输注后 6 个月以上。接受 mRNA 疫苗接种的 MS 患者 COVID-19 住院的绝对风险较低,不应排除使用利妥昔单抗,因为它与其他 DMT 相比具有显著的疗效、成本和便利性优势。