Verghese Dhiran, Manubolu Sanjay, Budoff Matthew J
Section of Advanced Cardiovascular Imaging, Division of Cardiovascular Medicine, Department of Medicine, Harbor-UCLA Medical Center, Torrance, California, USA.
Section of Cardiovascular Medicine, Department of Medicine, Lundquist Institute at Harbor UCLA Medical Center, Torrance, California, USA.
Am J Prev Cardiol. 2022 Nov 3;12:100427. doi: 10.1016/j.ajpc.2022.100427. eCollection 2022 Dec.
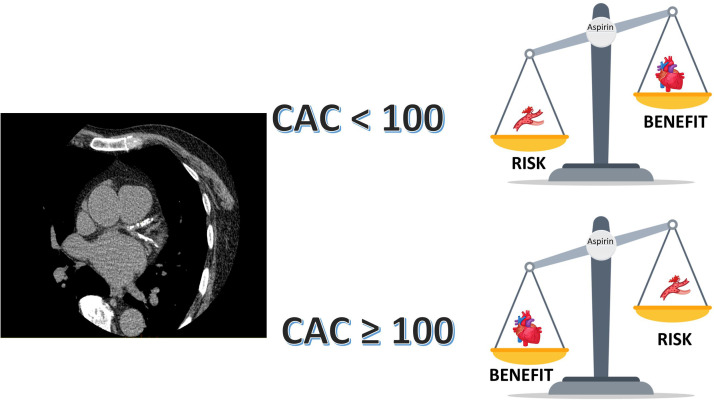
Aspirin has been a cornerstone for primary prevention of cardiovascular disease for decades, however its use in primary prevention has been challenged in recent years. The 2022 USPSTF guidelines lowered the recommendation for the use of aspirin in primary prevention based on the recent trials that demonstrated a low to neutral benefit and an increased bleeding risk with the use of aspirin in primary prevention. However, these trials enrolled patients at a relatively low risk for atherosclerotic cardiovascular disease (ASCVD) and higher bleeding risk which could have contributed to the negative results of the trials. ASCVD prevention is ideal when therapies are personalized based on individual risk. Coronary artery calcium (CAC) score is a robust marker of atherosclerosis and reliably predicts the ASCVD risk in a graded fashion. Several studies have demonstrated the use of a CAC≥100 to identify patients who will benefit from the use of aspirin in primary prevention. Furthermore, a CAC=0 identifies patients in whom aspirin would lead to net harm. In the continuum of risk from primary to secondary prevention, CAC is likely to identify the level of risk that warrants aspirin use in patients with subclinical ASCVD. The ACC/AHA 2019 primary prevention guidelines recommend the use of CAC to reclassify risk and guide personalized allocation of statins and aspirin. Although the USPSTF has not endorsed the use of CAC in the past, given an extensive body of evidence for use of CAC to guide primary preventive therapies including aspirin, it seems reasonable to use CAC to identify the level of plaque burden at which the benefit of aspirin outweighs its risk in clinical practice and personalize theallocation of aspirin in primary prevention. Future studies and randomized trials assessing the role of preventive therapies should use CAC score for risk stratification.
几十年来,阿司匹林一直是心血管疾病一级预防的基石,然而近年来其在一级预防中的应用受到了挑战。2022年美国预防服务工作组(USPSTF)指南基于近期试验降低了阿司匹林在一级预防中的使用推荐,这些试验表明阿司匹林在一级预防中的益处低至中性,且使用阿司匹林会增加出血风险。然而,这些试验纳入的是动脉粥样硬化性心血管疾病(ASCVD)风险相对较低且出血风险较高的患者,这可能是试验得出阴性结果的原因。当根据个体风险进行个性化治疗时,ASCVD预防是理想的。冠状动脉钙化(CAC)评分是动脉粥样硬化的有力标志物,并以分级方式可靠地预测ASCVD风险。多项研究表明,使用CAC≥100来识别将从阿司匹林一级预防中获益的患者。此外,CAC = 0可识别出使用阿司匹林会导致净危害的患者。在从一级预防到二级预防的连续风险中,CAC可能会确定在亚临床ASCVD患者中使用阿司匹林的风险水平。美国心脏病学会/美国心脏协会(ACC/AHA)2019年一级预防指南建议使用CAC来重新分类风险,并指导他汀类药物和阿司匹林的个性化分配。尽管USPSTF过去未认可使用CAC,但鉴于有大量证据表明使用CAC可指导包括阿司匹林在内的一级预防治疗,在临床实践中使用CAC来确定斑块负担水平,即阿司匹林的益处超过其风险的水平,并使阿司匹林在一级预防中的分配个性化似乎是合理的。未来评估预防治疗作用的研究和随机试验应使用CAC评分进行风险分层。