Transplantation and Clinical Virology, Department Biomedicine, University of Basel, Basel, Switzerland.
Clinical Virology, University Hospital Basel, Basel, Switzerland.
J Infect Dis. 2023 Apr 12;227(7):888-900. doi: 10.1093/infdis/jiac450.
High-level BK polyomavirus (BKPyV) replication in allogeneic hematopoietic cell transplantation (HCT) predicts failing immune control and BKPyV-associated hemorrhagic cystitis.
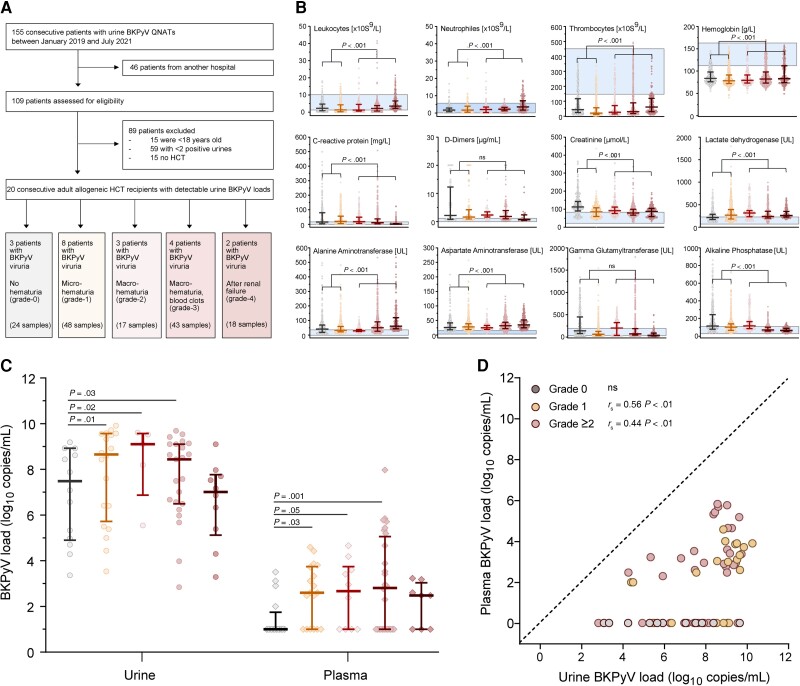
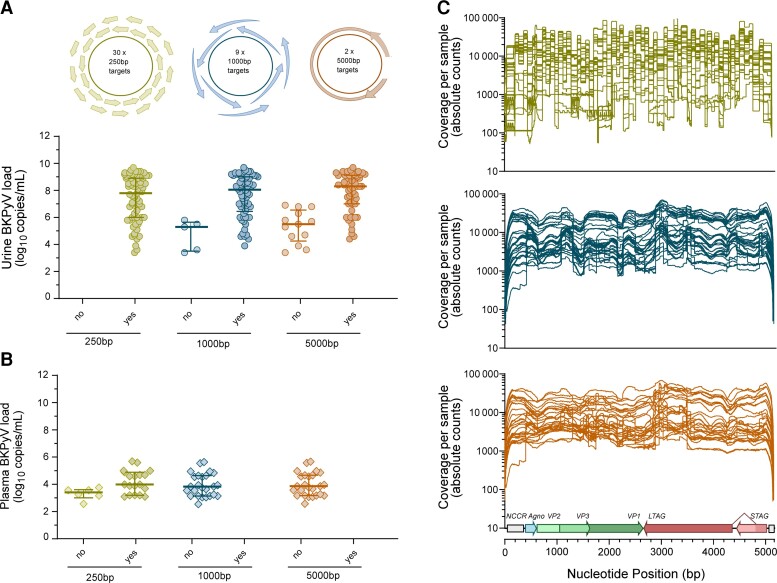
To identify molecular markers of BKPyV replication and disease, we scrutinized BKPyV DNA-loads in longitudinal urine and plasma pairs from 20 HCT patients using quantitative nucleic acid testing (QNAT), DNase-I treatment prior to QNAT, next-generation sequencing (NGS), and tested cell-mediated immunity.
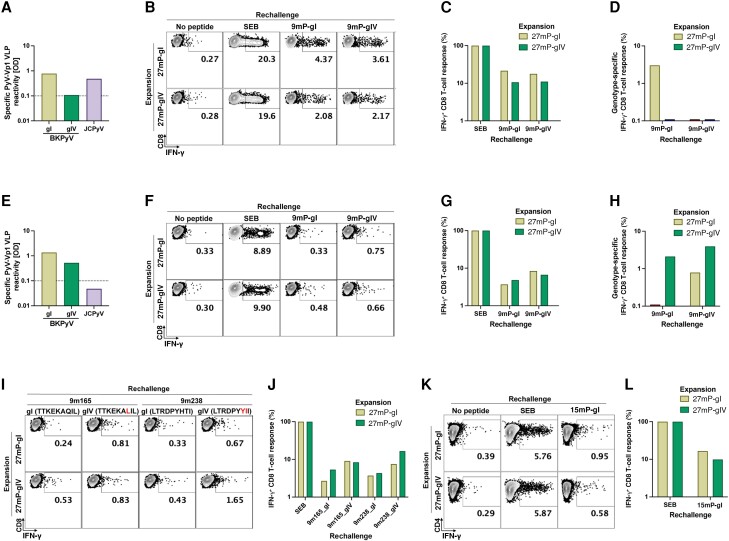
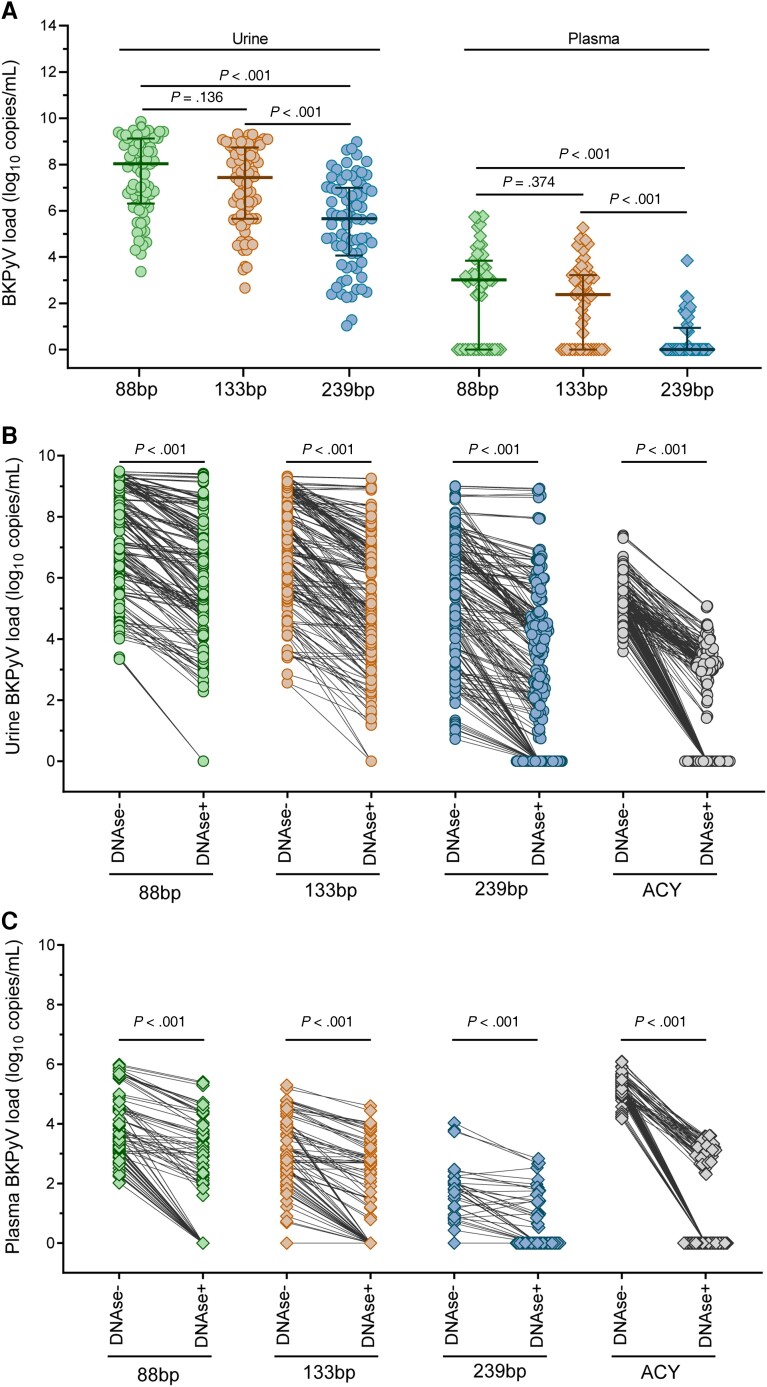
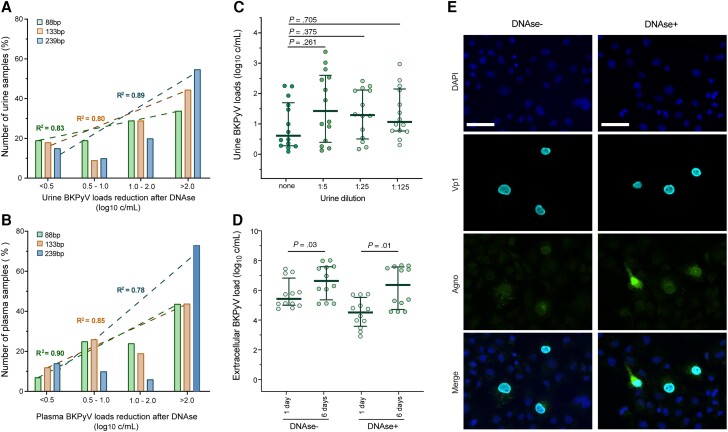
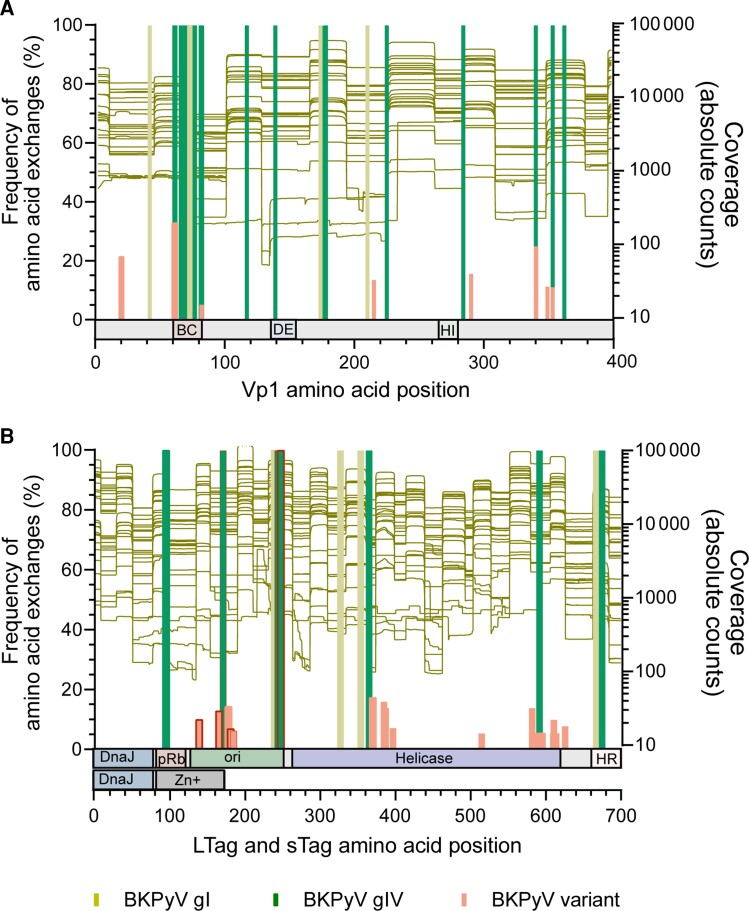
We found that larger QNAT amplicons led to under-quantification and false-negatives results (P < .001). DNase-I reduced urine and plasma BKPyV-loads by >90% (P < .001), indicating non-encapsidated BKPyV genomes. DNase-resistant urine BKPyV-loads remained infectious in cell culture. BKPyV genome fragmentation of ≤250 bp impaired NGS coverage of genetic variation using 1000-bp and 5000-bp amplicons. Conversely, 250-bp amplicons captured viral minority variants. We identified genotype-specific and genotype-independent changes in capsid Vp1 or T-antigen predicted to escape from antibody neutralization or cytotoxic CD8 T-cells, respectively. Genotype-specific changes in immunodominant 9mers were associated with reduced or absent CD8 T-cell responses. Thus, failure to control BKPyV replication in HCT Patients may involve insufficient genotype-specific cytotoxic CD8 T-cell responses, potentially predictable by low neutralizing antibodies as well as genotype-independent immune escape.
Our results provide new insights for patient evaluation and for designing immune protection through neutralizing antibodies, adoptive T-cell therapy, or vaccines.
同种异体造血细胞移植(HCT)中高水平 BK 多瘤病毒(BKPyV)复制预示着免疫控制失败和 BKPyV 相关出血性膀胱炎。
为了确定 BKPyV 复制和疾病的分子标志物,我们使用定量核酸检测(QNAT)、QNAT 前 DNase-I 处理、下一代测序(NGS)对 20 例 HCT 患者的纵向尿液和血浆对进行了 BKPyV DNA 载量分析,并检测了细胞介导的免疫。
我们发现更大的 QNAT 扩增子导致定量不足和假阴性结果(P<0.001)。DNase-I 降低了尿液和血浆 BKPyV 载量>90%(P<0.001),表明存在非囊封的 BKPyV 基因组。DNase 抗性尿液 BKPyV 载量在细胞培养中仍具有感染性。≤250bp 的 BKPyV 基因组片段会损害使用 1000bp 和 5000bp 扩增子进行遗传变异的 NGS 覆盖。相反,250bp 扩增子捕获病毒少数变体。我们发现了衣壳 Vp1 或 T 抗原的基因型特异性和基因型非特异性变化,分别预测逃避抗体中和或细胞毒性 CD8 T 细胞。免疫优势 9 mers 的基因型特异性变化与减少或缺失 CD8 T 细胞反应相关。因此,HCT 患者中 BKPyV 复制失控可能涉及细胞毒性 CD8 T 细胞反应不足,这可能可以通过低中和抗体以及基因型非特异性免疫逃逸来预测。
我们的研究结果为患者评估以及通过中和抗体、过继性 T 细胞治疗或疫苗设计提供了新的见解。