Jacobsson Susanne, Golparian Daniel, Oxelbark Joakim, Wicha Wolfgang W, da Costa Renata Maria Augusto, Franceschi Francois, Brown David, Louie Arnold, Gelone Steven P, Drusano George, Unemo Magnus
WHO Collaborating Centre for Gonorrhoea and Other STIs, National Reference Laboratory for Sexually Transmitted Infections, Department of Laboratory Medicine, Faculty of Medicine and Health, Örebro University, Örebro, Sweden.
Division of Clinical Chemistry, Department of Laboratory Medicine, Faculty of Medicine and Health, Örebro University, Örebro, Sweden.
Front Pharmacol. 2022 Nov 14;13:1035841. doi: 10.3389/fphar.2022.1035841. eCollection 2022.
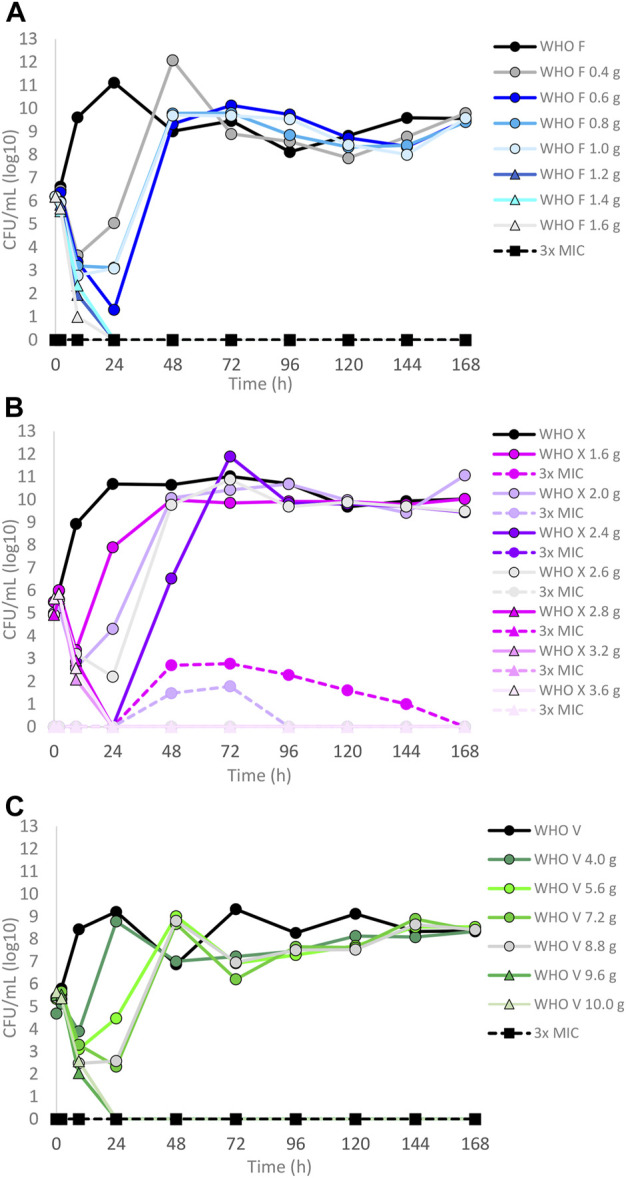
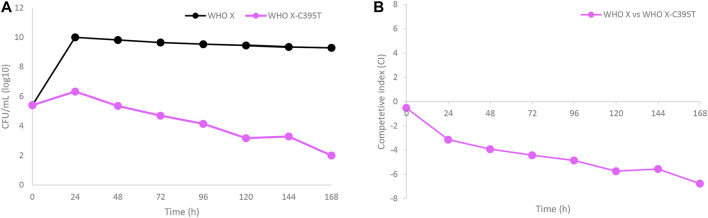
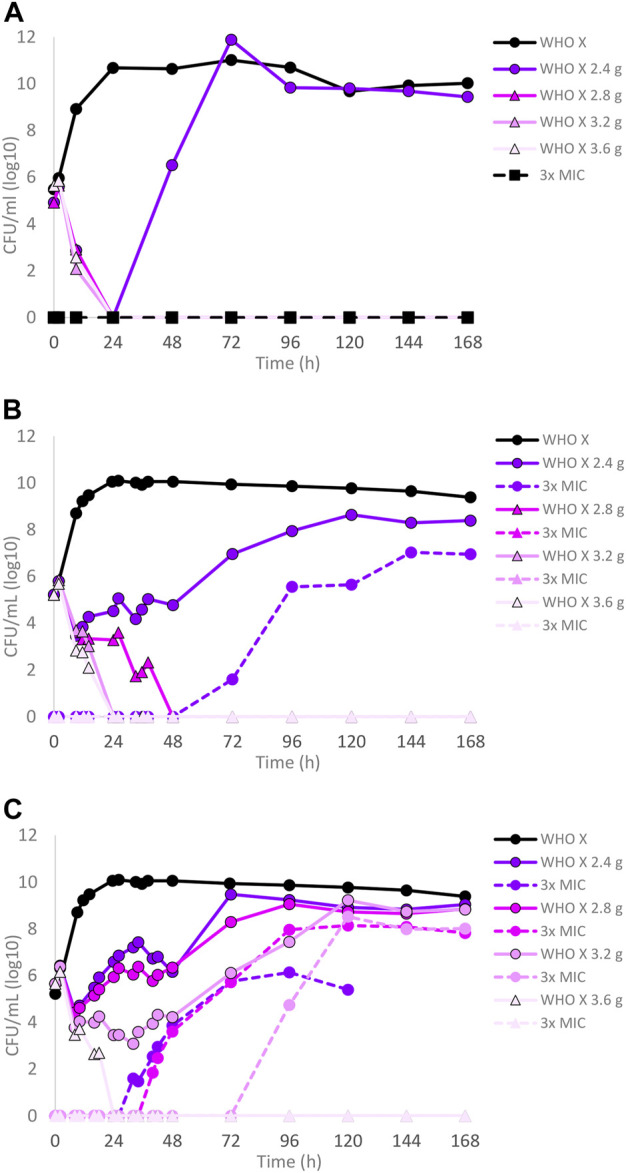
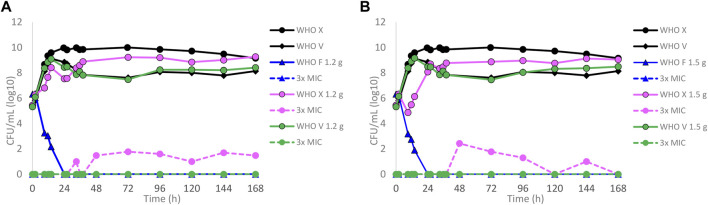
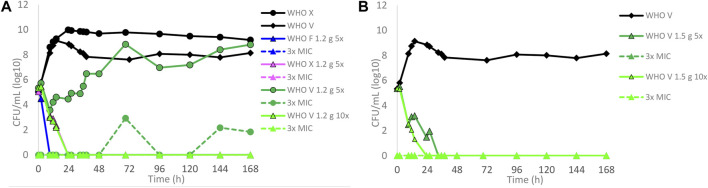
The emergence and spread of antimicrobial resistance in is seriously threatening the treatment and control of gonorrhea globally. Novel treatment options are essential, coupled with appropriate methods to pharmacodynamically examine the efficacy and resistance emergence of these novel drugs. Herein, we used our dynamic hollow fiber infection model (HFIM) to evaluate protein-unbound lefamulin, a semisynthetic pleuromutilin, against . Dose-range and dose-fractionation experiments with reference strains: WHO F (susceptible to all relevant antimicrobials), WHO X (extensively drug-resistant, including ceftriaxone resistance), and WHO V (high-level azithromycin resistant, and highest gonococcal MIC of lefamulin (2 mg/l) reported), were performed to examine lefamulin gonococcal killing and resistance development during treatment. The dose-range experiments, simulating a single oral dose of lefamulin based on human plasma concentrations, indicated that ≥1.2 g, ≥2.8 g, and ≥9.6 g of lefamulin were required to eradicate WHO F, X, and V, respectively. Dose-fractionation experiments, based on human lefamulin plasma concentrations, showed that WHO X was eradicated with ≥2.8 g per day when administered as q12 h (1.4 g twice a day) and with ≥3.6 g per day when administered as q8 h (1.2 g thrice a day), both for 7 days. However, when simulating the treatment with 5-10 times higher concentrations of free lefamulin in relevant gonorrhea tissues (based on urogenital tissues in a rat model), 600 mg every 12 h for 5 days (approved oral treatment for community-acquired bacterial pneumonia) eradicated all strains, and no lefamulin resistance emerged in the successful treatment arms. In many arms failing single or multiple dose treatments for WHO X, lefamulin-resistant mutants (MIC = 2 mg/l), containing an A132V amino acid substitution in ribosomal protein L3, were selected. Nevertheless, these lefamulin-resistant mutants demonstrated an impaired biofitness. In conclusion, a clinical study is warranted to elucidate the clinical potential of lefamulin as a treatment option for uncomplicated gonorrhea (as well as several other bacterial STIs).
抗菌药物耐药性在淋球菌中的出现和传播正严重威胁着全球淋病的治疗和控制。新型治疗方案至关重要,同时还需要有适当的方法从药效学角度来检验这些新药的疗效及耐药性的产生。在此,我们使用动态中空纤维感染模型(HFIM)来评估蛋白未结合型的左法莫林(一种半合成截短侧耳素)对淋球菌的作用。我们用参考菌株进行了剂量范围和剂量分割实验,这些参考菌株包括:世界卫生组织F株(对所有相关抗菌药物敏感)、世界卫生组织X株(广泛耐药,包括对头孢曲松耐药)以及世界卫生组织V株(对阿奇霉素高水平耐药,且报道的左法莫林对淋球菌的最高最低抑菌浓度(MIC)为2mg/L),以检验治疗期间左法莫林对淋球菌的杀灭作用及耐药性的产生情况。剂量范围实验基于人体血浆浓度模拟单次口服左法莫林,结果表明,分别需要≥1.2g、≥2.8g和≥9.6g的左法莫林才能根除世界卫生组织F株、X株和V株。基于人体左法莫林血浆浓度的剂量分割实验表明,世界卫生组织X株在按q12h(每日两次,每次1.4g)给药时,每日≥2.8g可被根除;按q8h(每日三次,每次1.2g)给药时,每日≥3.6g,持续7天可被根除。然而,当在相关淋病组织中模拟使用比游离左法莫林高5至10倍浓度的药物治疗时(基于大鼠模型中的泌尿生殖组织),每12小时600mg,持续5天(社区获得性细菌性肺炎的批准口服治疗方案)可根除所有菌株,且在成功治疗组中未出现左法莫林耐药性。在许多针对世界卫生组织X株的单剂量或多剂量治疗失败的组中,选择出了含有核糖体蛋白L3中A132V氨基酸替代的左法莫林耐药突变体(MIC = 2mg/L)。然而,这些左法莫林耐药突变体表现出生物学适应性受损。总之,有必要开展一项临床研究来阐明左法莫林作为单纯性淋病(以及其他几种细菌性性传播感染)治疗选择的临床潜力。