Uppsala Monitoring Centre, Uppsala, Sweden.
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Drug Saf. 2023 Feb;46(2):109-120. doi: 10.1007/s40264-022-01258-0. Epub 2022 Dec 5.
Signals of adverse drug reactions (ADRs) can be supported by reports of ADRs and by interventional and non-interventional studies. The evidence base and features of ADR reports that are used to support signals remain to be comprehensively described. To this end, we have undertaken a scoping review.
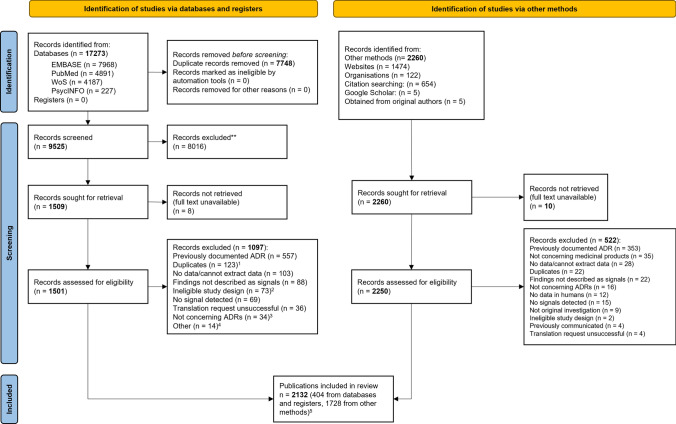
We searched the following databases: PubMed, EMBASE, PsycINFO, Web of Science, and Google Scholar, without language or time restrictions. We also hand searched the bibliographies of relevant studies. We included studies of any design if the results were described as signals. We assessed the levels of evidence using the Oxford Centre for Evidence-Based Medicine (OCEBM) criteria and coded features of reports of ADRs using the Bradford Hill guidelines.
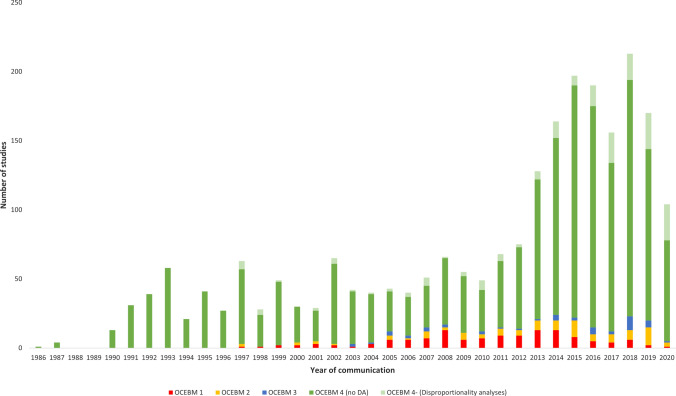
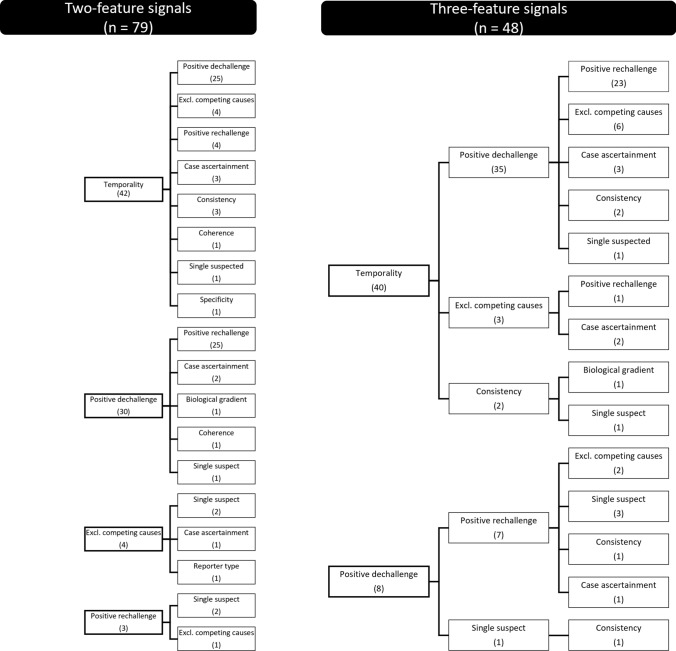
Overall, 1974 publications reported 2421 studies of signals; 1683/2421 were clinical assessments of anecdotal reports of ADRs, but only 225 (13%) of these included explicit judgments on which features of the ADR reports were supportive of a signal. These 225 studies yielded 228 signals; these were supported by features, which were: 'experimental evidence' (i.e., positive dechallenge or rechallenge, 154 instances [68%]), 'temporality' (i.e., time to onset, 130 [57%]), 'exclusion of competing causes' (49 [21%]), and others (40 [17%]). Positive dechallenge/rechallenge often co-occurred with temporality (77/228). OCEBM 4 (i.e., case series and case-control studies) was the most frequent level of evidence (2078 studies). Between 2013 and 2019, there was a three-fold increase in clinical assessments of reports of ADRs compared with a less than two-fold increase in studies supported by higher levels of evidence (i.e., OCEBM 1-3). We identified an increased rate between 2013 and 2019 in disproportionality analyses (about 15 studies per year), mostly from academia.
Most signals were supported by temporality and dechallenge/rechallenge, but clear reporting of judgments on causality remains infrequent. The number of studies supported only by anecdotal reports of ADRs increased from year to year. The impact of a growing number of signals of disproportionate reporting communicated without an accompanying clinical assessment should be evaluated.
药物不良反应(ADR)的信号可以通过 ADR 报告和干预性及非干预性研究来支持。用于支持信号的 ADR 报告的证据基础和特征仍有待全面描述。为此,我们进行了范围界定审查。
我们在没有语言和时间限制的情况下,在以下数据库中进行了检索:PubMed、EMBASE、PsycINFO、Web of Science 和 Google Scholar,还手动检索了相关研究的参考文献。如果结果被描述为信号,则纳入任何设计的研究。我们使用牛津循证医学中心(OCEBM)标准评估证据水平,并使用布拉德福德-希尔指南对 ADR 报告的特征进行编码。
总体而言,有 1974 篇出版物报告了 2421 项信号研究;其中 1683/2421 项为对 ADR 传闻报告的临床评估,但只有 225 项(13%)明确判断了 ADR 报告的哪些特征支持信号。这 225 项研究产生了 228 个信号;这些信号得到了以下特征的支持:“实验证据”(即阳性撤药或再挑战,154 例[68%])、“时间性”(即发病时间,130 例[57%])、“排除竞争原因”(49 例[21%])和其他特征(40 例[17%])。阳性撤药/再挑战常常与时间性同时出现(228 例中的 77 例)。OCEBM 4 级(即病例系列和病例对照研究)是最常见的证据水平(2078 项研究)。与证据水平较高(即 OCEBM 1-3)的研究相比,2013 年至 2019 年,对 ADR 报告的临床评估增加了两倍多,而支持这些研究的报告则增加了不到两倍。我们发现,2013 年至 2019 年,比例失调分析的速度加快(每年约 15 项研究),主要来自学术界。
大多数信号得到了时间性和撤药/再挑战的支持,但对因果关系的判断仍很少明确报告。仅基于 ADR 传闻报告的研究数量逐年增加。应评估越来越多的不成比例报告信号的传播,而没有伴随临床评估的影响。