College of Engineering and Engineering Technology, Northern Illinois University, DeKalb, IL, USA.
School of Interdisciplinary Health Professions, Northern Illinois University, DeKalb, IL, USA.
BMC Cancer. 2022 Dec 6;22(1):1275. doi: 10.1186/s12885-022-10370-4.
This study constructs a lung cancer risk index (LCRI) that incorporates many modifiable risk factors using an easily reproducible and adaptable method that relies on publicly available data.
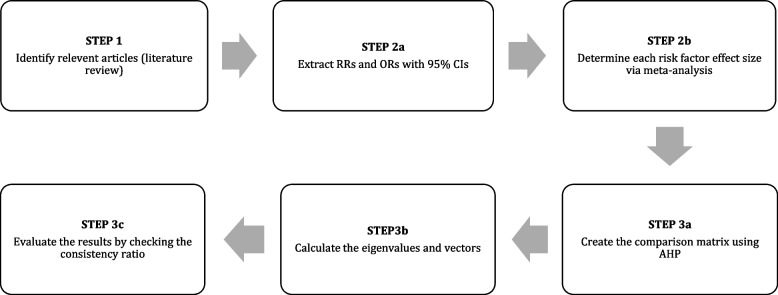
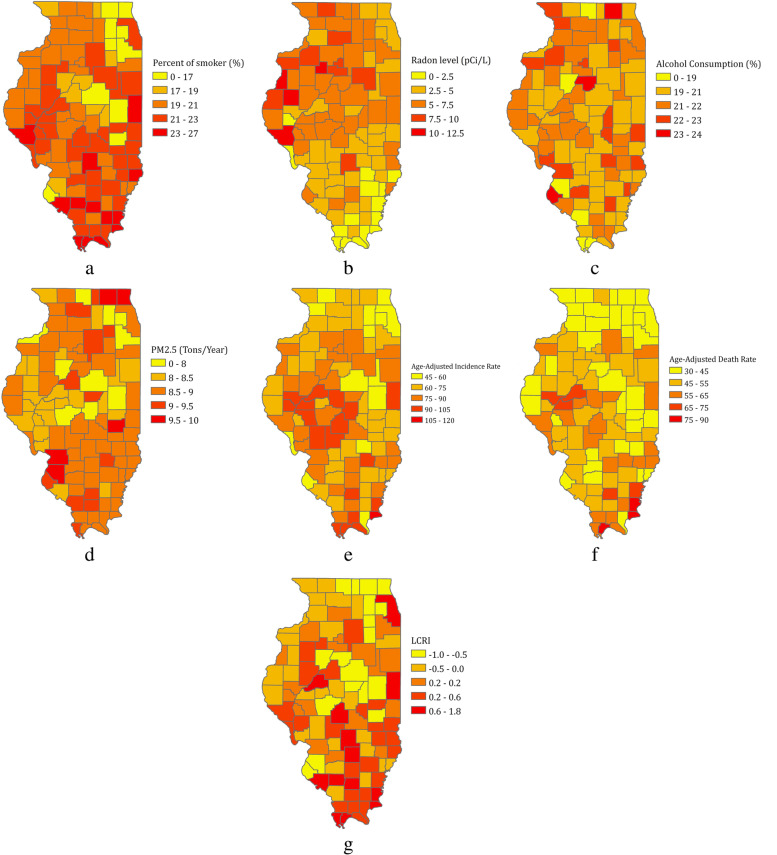
We used meta-analysis followed by Analytic Hierarchy Process (AHP) to generate a lung cancer risk index (LCRI) that incorporates seven modifiable risk factors (active smoking, indoor air pollution, occupational exposure, alcohol consumption, secondhand smoke exposure, outdoor air pollution, and radon exposure) for lung cancer. Using county-level population data, we then performed a case study in which we tailored the LCRI for use in the state of Illinois (LCRI).
For both the LCRI and the LCRI, active smoking had the highest weights (46.1% and 70%, respectively), whereas radon had the lowest weights (3.0% and 5.7%, respectively). The weights for alcohol consumption were 7.8% and 14.7% for the LCRI and the LCRI, respectively, and were 3.8% and 0.95% for outdoor air pollution. Three variables were only included in the LCRI: indoor air pollution (18.5%), occupational exposure (13.2%), and secondhand smoke exposure (7.6%). The Consistency Ratio (CR) was well below the 0.1 cut point. The LCRI was moderate though significantly correlated with age-adjusted lung cancer incidence (r = 0.449, P < 0.05) and mortality rates (r = 0.495, P < 0.05).
This study presents an index that incorporates multiple modifiable risk factors for lung cancer into one composite score. Since the LCRI allows data comprising the composite score to vary based on the location of interest, this measurement tool can be used for any geographic location where population-based data for individual risk factors exist. Researchers, policymakers, and public health professionals may utilize this framework to determine areas that are most in need of lung cancer-related interventions and resources.
本研究构建了一个肺癌风险指数(LCRI),该指数采用易于复制和适应的方法,结合了许多可改变的风险因素,这些因素依赖于公开可用的数据。
我们使用荟萃分析和层次分析法(AHP)来生成一个肺癌风险指数(LCRI),该指数纳入了 7 个可改变的风险因素(主动吸烟、室内空气污染、职业暴露、饮酒、二手烟暴露、室外空气污染和氡暴露)。然后,我们使用县级人口数据进行了一项案例研究,根据伊利诺伊州的情况对 LCRI 进行了调整(LCRI)。
对于 LCRI 和 LCRI,主动吸烟的权重最高(分别为 46.1%和 70%),而氡的权重最低(分别为 3.0%和 5.7%)。饮酒的权重分别为 LCRI 的 7.8%和 LCRI 的 14.7%,而室外空气污染的权重分别为 3.8%和 0.95%。只有三个变量被纳入 LCRI:室内空气污染(18.5%)、职业暴露(13.2%)和二手烟暴露(7.6%)。一致性比率(CR)远低于 0.1 的临界值。LCRI 适中,但与年龄调整后的肺癌发病率(r=0.449,P<0.05)和死亡率(r=0.495,P<0.05)显著相关。
本研究提出了一个将多个肺癌可改变风险因素纳入一个综合评分的指数。由于 LCRI 允许基于感兴趣的位置改变包含综合评分的数据,因此该测量工具可用于存在个体风险因素的人群数据的任何地理位置。研究人员、政策制定者和公共卫生专业人员可以利用这一框架来确定最需要肺癌相关干预措施和资源的地区。