Knitschke Michael, Yonan Magdalena, Roller Fritz Christian, Pons-Kühnemann Jörn, Attia Sameh, Howaldt Hans-Peter, Streckbein Philipp, Böttger Sebastian
Department of Oral and Maxillofacial Surgery, Justus-Liebig-University, Klinikstrasse 33, 35392 Giessen, Germany.
Department of Diagnostic and Interventional Radiology and Pediatric Radiology, Justus-Liebig-University, Klinikstrasse 33, 35392 Giessen, Germany.
Cancers (Basel). 2022 Nov 24;14(23):5774. doi: 10.3390/cancers14235774.
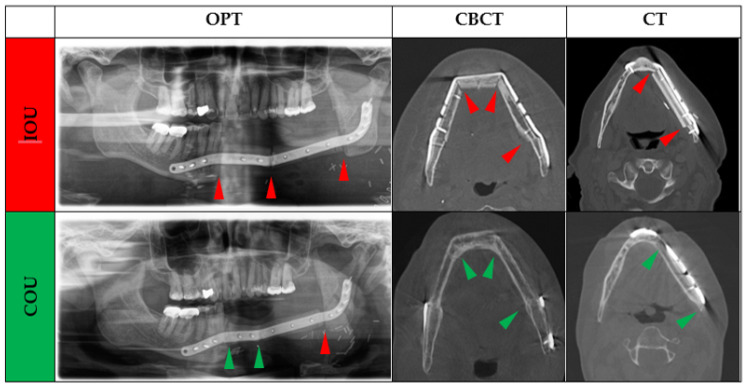
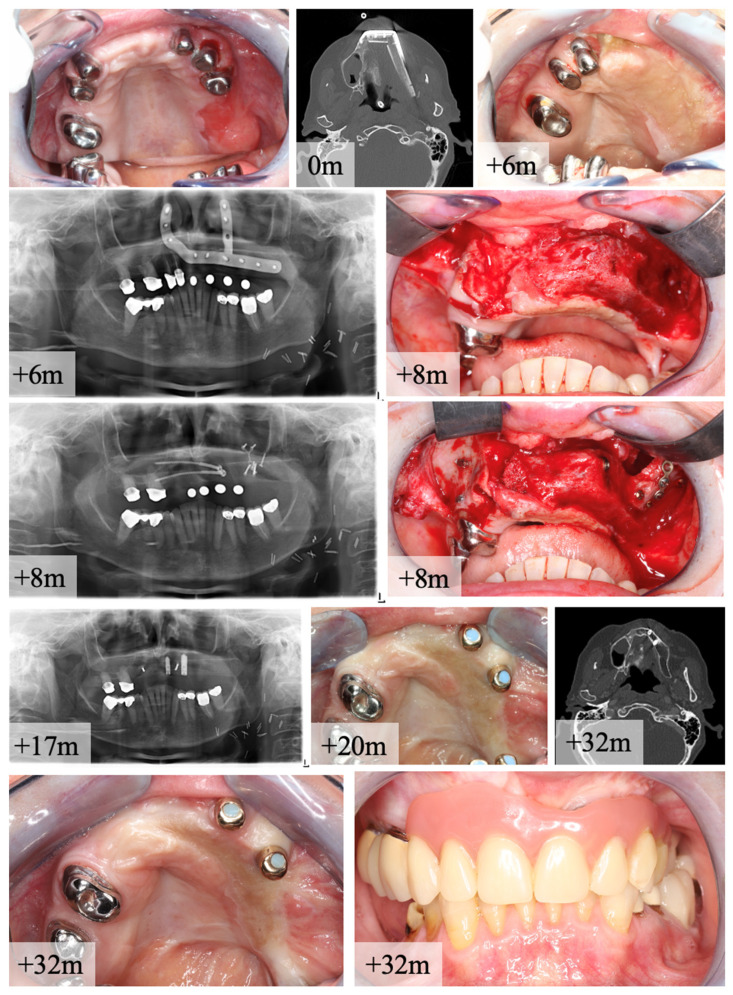
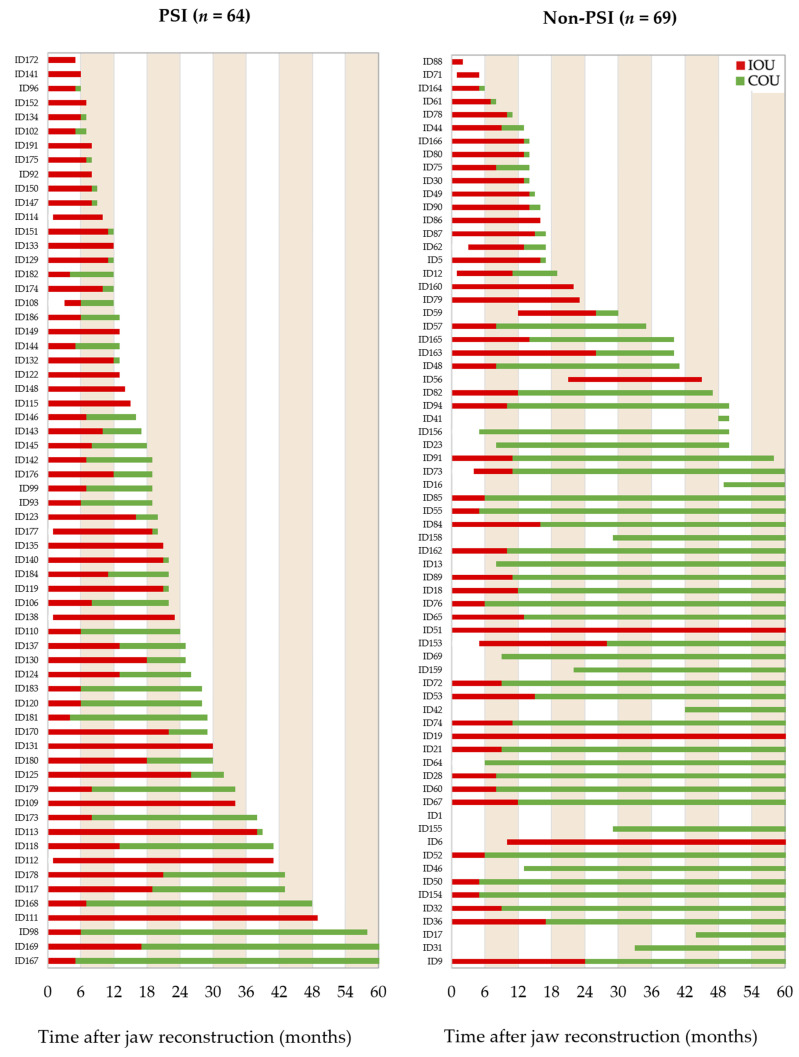
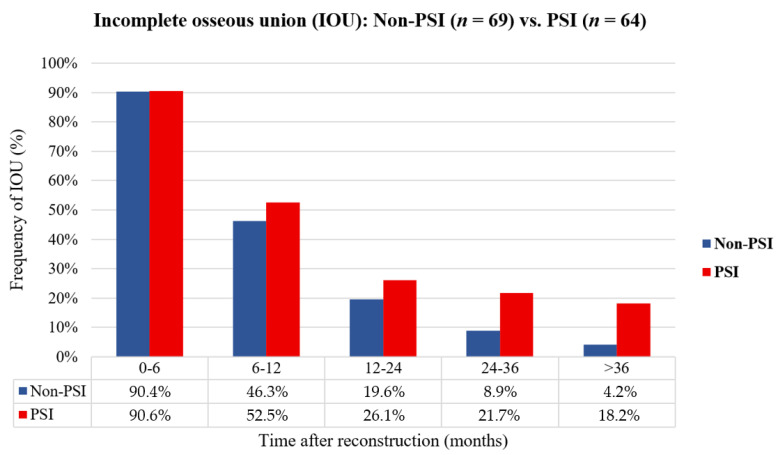
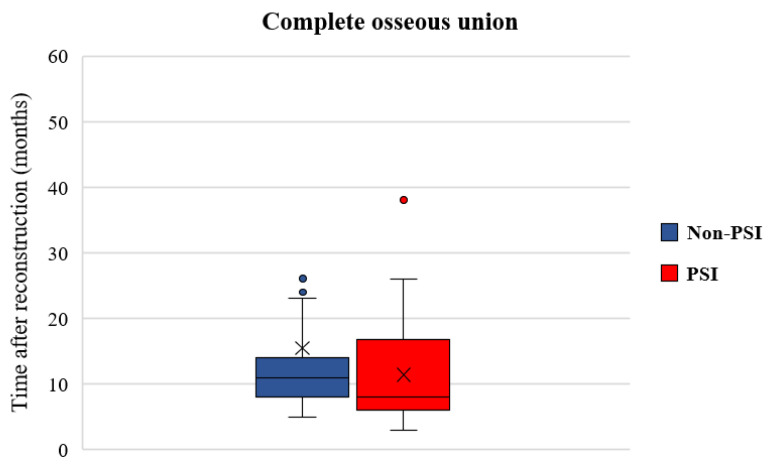
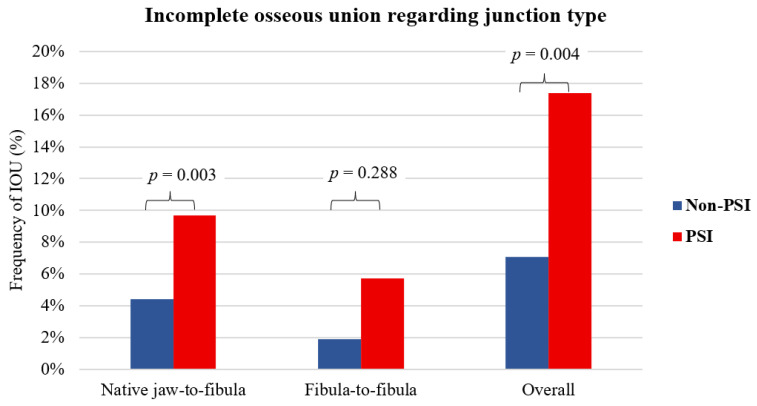
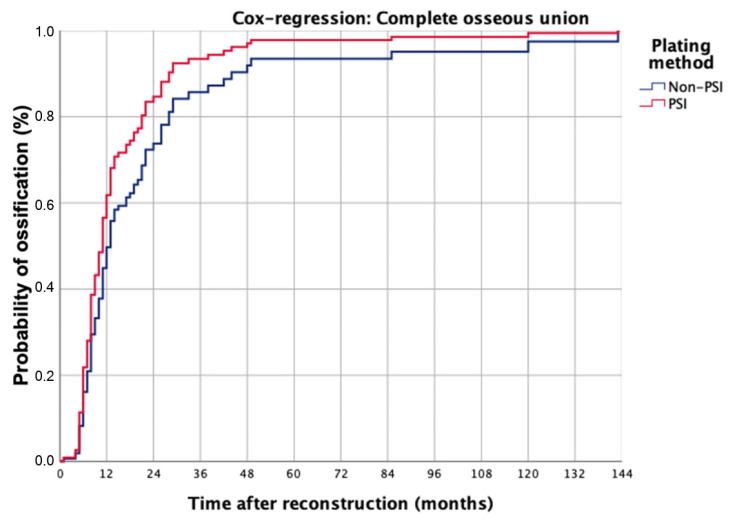
This is a monocentric, retrospective study of patients who underwent successful immediate or delayed maxilla or mandible reconstructions with FFF from January 2005 to December 2021. Panoramic radiograph, computed tomography scans, and cone-beam CTs were analyzed concerning the osseous union of the intersegmental junctions between maxillary or mandibular native jaw and fibular bone. The primary parameter was to estimate the status of osseous union according to osteosynthesis type. A total number of 133 patients (PSI: n = 64, non-PSI: n = 69) were included in the present study. The mean age was 56.7 ± 14.0 (Range: 14.7−82.7); the primary diagnosis was in 105 patients a malignant (78.9%) and in 20 patients a benign (15.0%) tumor. Mandible reconstruction was performed on 103 patients (77.4%), and on 30 patients (22.6%), maxilla reconstruction was performed. The radiographic images provided a rate of incomplete osseous union (IOU) of about 90% in both groups in the first 6 months. Imaging between 6 and 12 months reveals an IOU rate in the non-PSI group of 46.3% vs. 52.5% in the PSI group, between 12 and 24 months, an IOU rate of 19.6% vs. 26.1%, between 24 and 36 months 8.9% vs. 21.7%, and after 36 months the IOU rate decreases to 4.2% vs. 18.2%. Multivariate logistic regression shows that only osteosynthesis type (OR = 3.518 [95%-CI = 1.223−10.124], p = 0.02) and adjuvant radiotherapy (OR = 4.804 [95%-CI = 1.602−14.409], p = 0.005) are independent risk factors for incomplete osseous union. Cox regression revealed that the variables plate-system (Hazard ratio, HR = 5.014; 95 %-CI: 1.826−3.769; p = 0.002) and adjuvant radiotherapy (HR = 5.710; 95 %-CI: 2.066−15.787; p < 0.001) are predictors for incomplete osseous union. In our study, the rate of incomplete bony fusion was significantly higher in the PSI group. Jaw-to-fibula apposition zones were significantly more affected than intersegmental zones. In multivariate analysis, a combination of osteosynthesis with PSI and adjuvant radiotherapy could be identified as a risk constellation for incomplete ossification.
这是一项单中心回顾性研究,研究对象为2005年1月至2021年12月期间接受游离腓骨瓣即刻或延期上颌骨或下颌骨重建且手术成功的患者。对全景X线片、计算机断层扫描及锥形束CT进行分析,观察上颌骨或下颌骨天然颌骨与腓骨之间节段间连接部位的骨愈合情况。主要参数是根据骨固定类型评估骨愈合状态。本研究共纳入133例患者(加压钢板内固定组:n = 64,非加压钢板内固定组:n = 69)。平均年龄为56.7±14.0岁(范围:14.7 - 82.7岁);105例患者(78.9%)的初步诊断为恶性肿瘤,20例患者(15.0%)为良性肿瘤。103例患者(77.4%)接受了下颌骨重建,30例患者(22.6%)接受了上颌骨重建。在前6个月,两组的影像学检查显示不完全骨愈合率约为90%。6至12个月的影像学检查显示,非加压钢板内固定组的不完全骨愈合率为46.3%,加压钢板内固定组为52.5%;12至24个月时,不完全骨愈合率分别为19.6%和26.1%;24至36个月时,分别为8.9%和*21.7%;36个月后,不完全骨愈合率降至4.2%和18.2%。多因素逻辑回归分析显示只有骨固定类型(比值比,OR = 3.518 [95%置信区间 = 1.223 - 10.124],p = 0.02)和辅助放疗(OR = 4.804 [95%置信区间 = 1.602 - 14.409],p = 0.005)是不完全骨愈合的独立危险因素。Cox回归分析显示,钢板系统变量(风险比,HR = 5.014;95%置信区间:1.826 - 3.769;p = 0.002)和辅助放疗(HR = 5.710;95%置信区间:2.066 - 15.787;p < 0.001)是不完全骨愈合的预测因素。在我们的研究中,加压钢板内固定组的不完全骨融合率明显更高。颌骨与腓骨贴合区域比节段间区域受影响更显著。在多因素分析中,加压钢板内固定联合骨固定与辅助放疗可被确定为不完全骨化的风险组合。