Antúnez-Conde Raúl, Salmerón José Ignacio, Díez-Montiel Alberto, Agea Marc, Gascón Dafne, Sada Ángela, Navarro Cuéllar Ignacio, Tousidonis Manuel, Ochandiano Santiago, Arenas Gema, Navarro Cuéllar Carlos
Maxillofacial Surgery Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
Front Oncol. 2021 Oct 5;11:719712. doi: 10.3389/fonc.2021.719712. eCollection 2021.
Vertical discrepancy between the fibula flap and the native mandible results in difficult prosthetic rehabilitation. The aim of this study was to evaluate the outcomes of 3D reconstruction of the mandible in oncologic patients using three different techniques through virtual surgical planning (VSP), cutting guides, customized titanium mesh and plates with CAD/CAM technology, STL models and intraoperative dynamic navigation for implant placement. Material and methods.
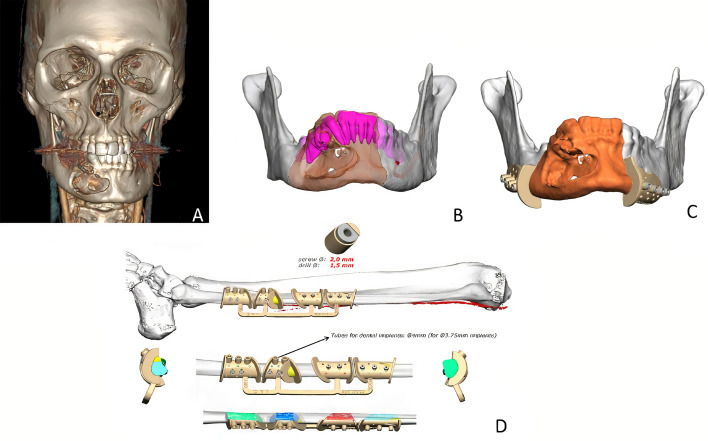
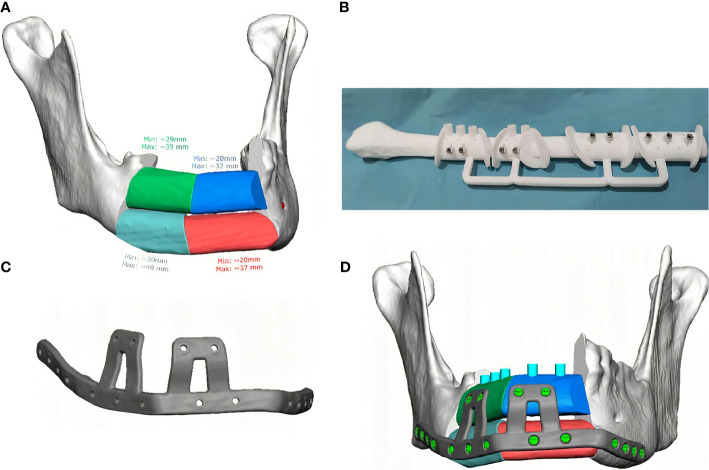
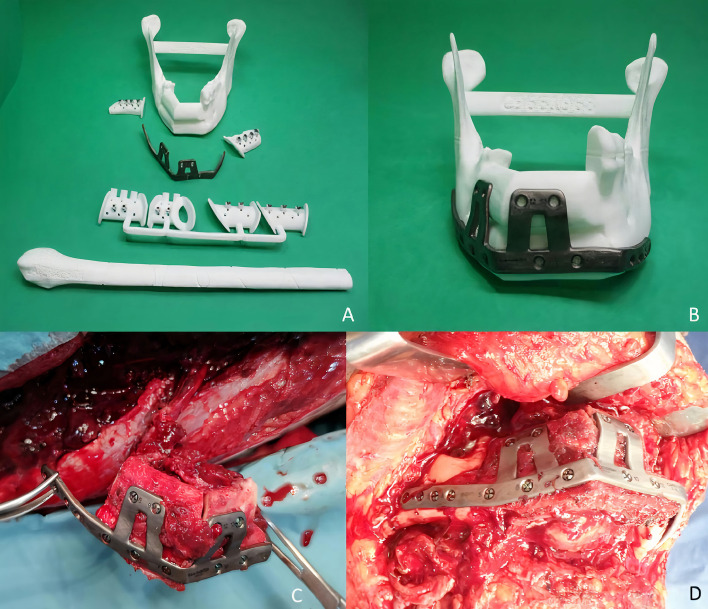
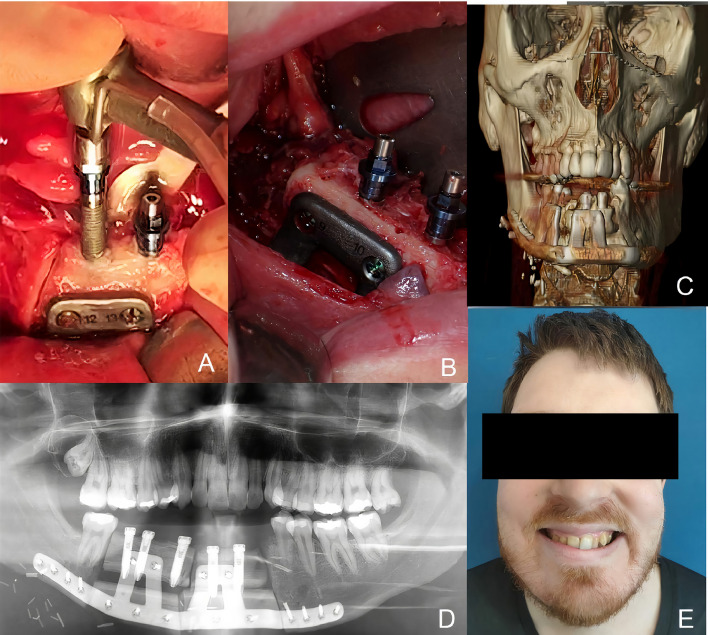
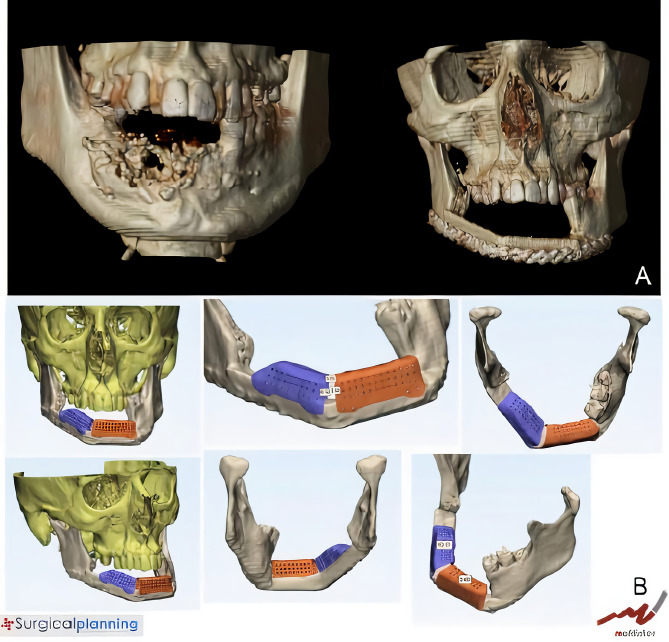
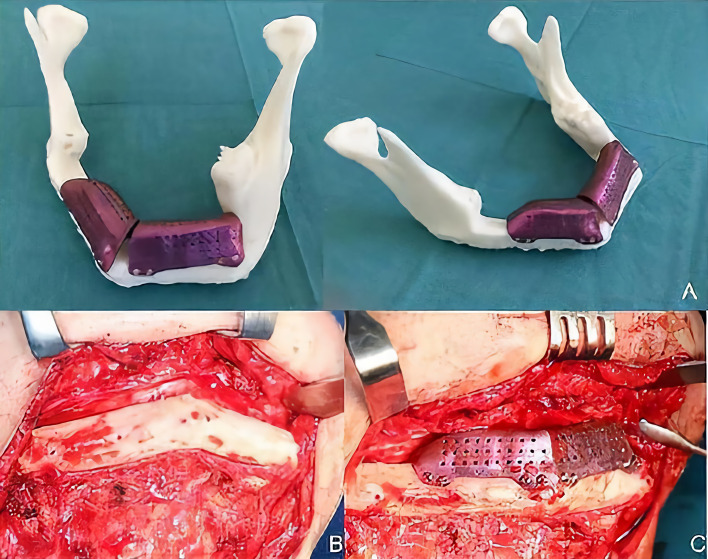
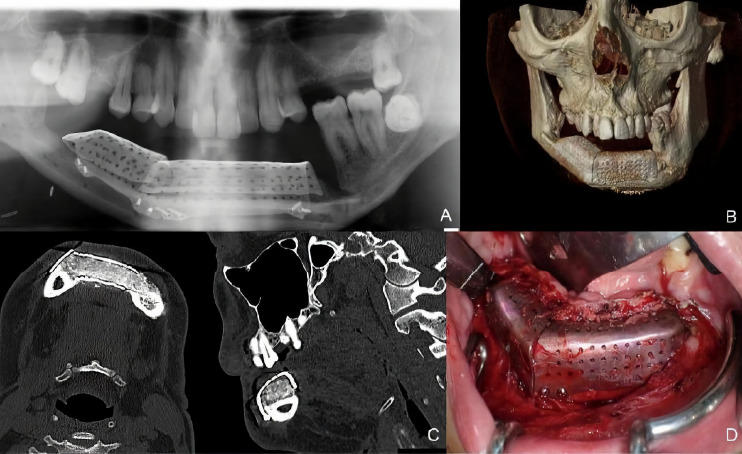
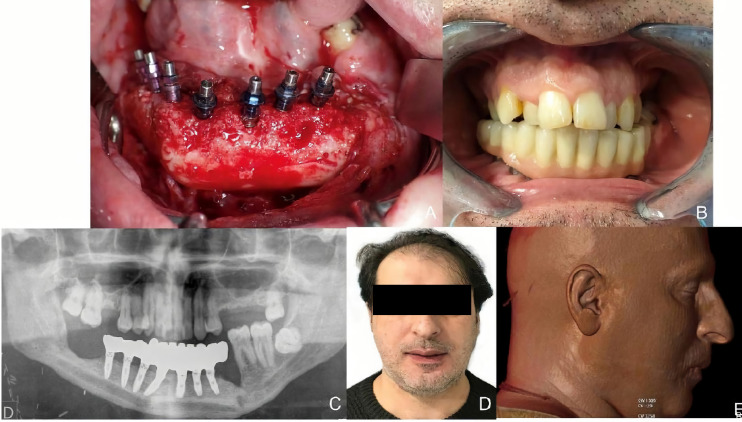
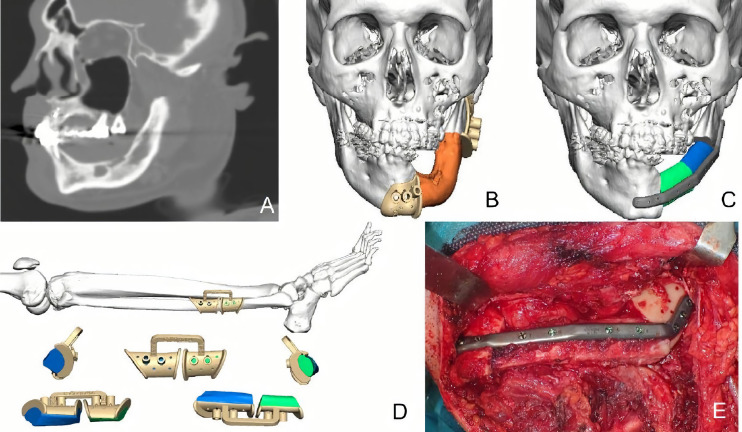
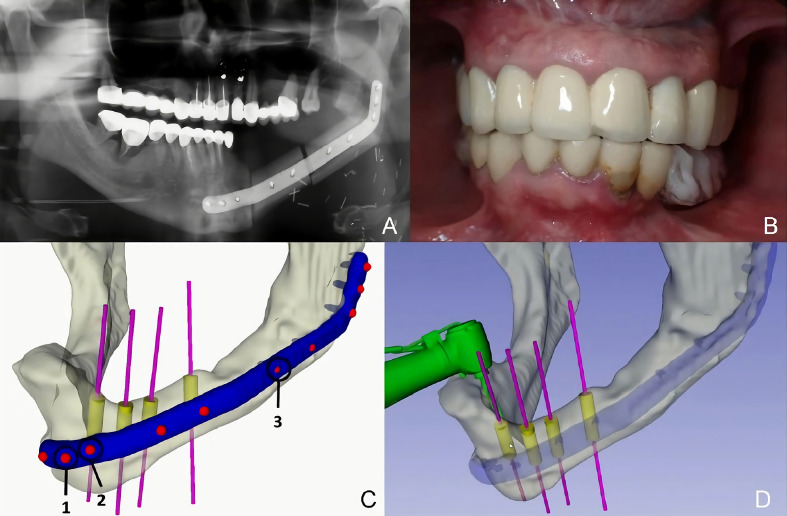
Three different techniques for mandibular reconstruction and implant rehabilitation were performed in 14 oncologic patients. Five patients (36%) underwent VSP, cutting guides, STL models and a customized double-barrel titanium plate with a double-barrel flap and immediate implants. In six patients (43%), VSP, STL models and a custom-made titanium mesh (CAD/CAM) for 3D reconstruction with iliac crest graft over a fibula flap with deferred dental implants were performed. Three patients (21%) underwent VSP with cutting guides and customized titanium plates for mandibular reconstruction and implant rehabilitation using intraoperative dynamic navigation was accomplished. Vertical bone reconstruction, peri-implant bone resorption, implant success rate, effects of radiotherapy in vertical reconstruction, bone resorption and implant failure, mastication, aesthetic result and dysphagia were evaluated.
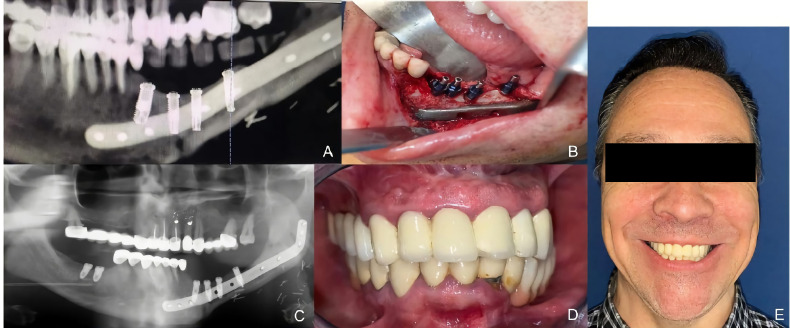
Significant differences in bone growth between the double-barrel technique and iliac crest graft with titanium mesh technique were found (p<0.002). Regarding bone resorption, there were no significant differences between the techniques (p=0.11). 60 implants were placed with an osseointegration rate of 91.49%. Five implants were lost during the osseointegration period (8%). Peri-implant bone resorption was measured with a mean of 1.27 mm. There was no significant difference between the vertical gain technique used and implant survival (p>0.385). Implant survival rates were higher in non-irradiated patients (p<0.017). All patients were rehabilitated with a fixed implant-supported prosthesis reporting a regular diet (80%), normal swallowing (85.7%) and excellent aesthetic results.
Multi-stage implementation of VSP, STL models and cutting guides, CAD/CAM technology, customized plates and in-house dynamic implant navigation for mandibular defects increases bone-to-bone contact, resolves vertical discrepancy and improves operative efficiency with reduced complication rates and minimal bone resorption. It provides accurate reconstruction that optimizes implant placement, thereby improving facial symmetry, aesthetics and function.
腓骨瓣与天然下颌骨之间的垂直差异导致修复假体困难。本研究的目的是通过虚拟手术规划(VSP)、切割导板、定制钛网和钢板,利用CAD/CAM技术、STL模型以及术中动态导航进行种植体植入,评估三种不同技术对肿瘤患者下颌骨进行三维重建的效果。材料与方法。
对14例肿瘤患者采用三种不同的下颌骨重建和种植体修复技术。5例患者(36%)接受了VSP、切割导板、STL模型以及定制的双筒钛板,采用双筒瓣和即刻种植体。6例患者(43%)接受了VSP、STL模型以及定制钛网(CAD/CAM)进行三维重建,在腓骨瓣上采用髂嵴移植并延期种植牙。3例患者(21%)接受了VSP并使用切割导板和定制钛板进行下颌骨重建和种植体修复,术中采用动态导航完成。评估垂直骨重建、种植体周围骨吸收、种植体成功率、放疗对垂直重建、骨吸收和种植体失败的影响、咀嚼、美学效果和吞咽困难情况。
发现双筒技术与钛网髂嵴移植技术之间在骨生长方面存在显著差异(p<0.002)。关于骨吸收,各技术之间无显著差异(p=0.11)。共植入60枚种植体,骨结合率为91.49%。在骨结合期有5枚种植体丢失(8%)。种植体周围骨吸收的平均测量值为1.27mm。所采用的垂直增高技术与种植体存留率之间无显著差异(p>0.385)。未接受放疗患者的种植体存留率更高(p<0.017)。所有患者均采用固定种植体支持的假体进行修复,报告饮食正常(80%)、吞咽正常(85.7%)且美学效果良好。
对下颌骨缺损采用VSP、STL模型和切割导板、CAD/CAM技术、定制钢板以及术中动态种植体导航的多阶段实施,可增加骨与骨的接触,解决垂直差异,提高手术效率,降低并发症发生率并减少骨吸收。它提供了精确的重建,优化了种植体植入,从而改善面部对称性、美学和功能。