Maznyczka Annette M, Matthews Connor J, Blaxill Jonathan M, Greenwood John P, Mozid Abdul M, Rossington Jennifer A, Veerasamy Murugapathy, Wheatcroft Stephen B, Curzen Nick, Bulluck Heerajnarain
Yorkshire Heart Centre, Leeds General Infirmary, Leeds Teaching Hospitals NHS Trust, Leeds LS1 3EX, UK.
Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds LS1 3EX, UK.
J Clin Med. 2022 Nov 30;11(23):7092. doi: 10.3390/jcm11237092.
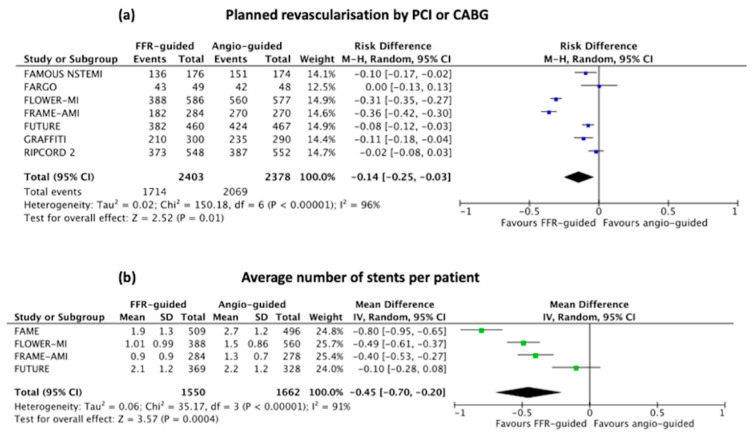
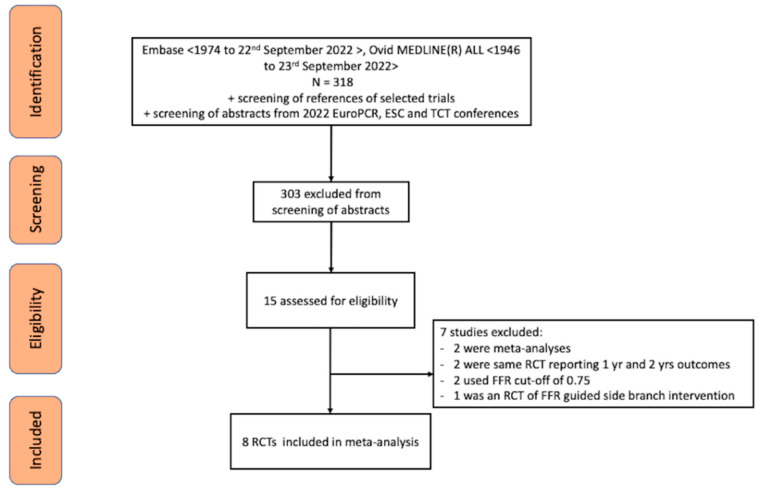
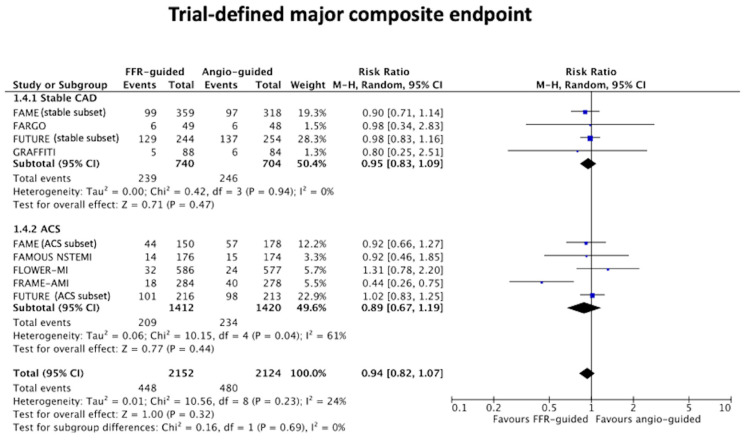
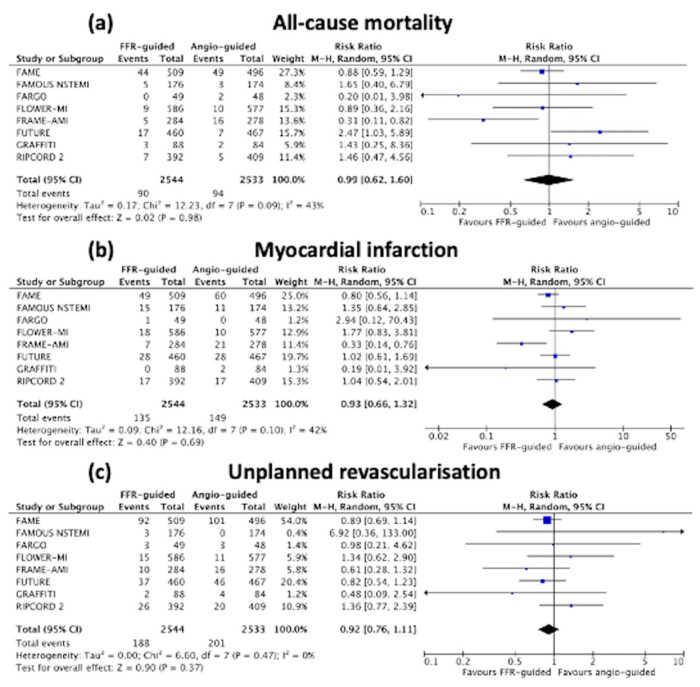
Background and Aims: Randomised controlled trials (RCTs) comparing outcomes after fractional flow reserve (FFR)-guided versus angiography-guided management for obstructive coronary artery disease (CAD) have produced conflicting results. We investigated the efficacy and safety of an FFR-guided versus angiography-guided management strategy among patients with obstructive CAD. Methods: A systematic electronic search of the major databases was performed from inception to September 2022. We included studies of patients presenting with angina or myocardial infarction (MI), managed with medications, percutaneous coronary intervention, or bypass graft surgery. A meta-analysis was performed by pooling the risk ratio (RR) using a random-effects model. The endpoints of interest were all-cause mortality, MI and unplanned revascularisation. Results: Eight RCTs, with outcome data from 5077 patients, were included. The weighted mean follow up was 22 months. When FFR-guided management was compared to angiography-guided management, there was no difference in all-cause mortality [3.5% vs. 3.7%, RR: 0.99 (95% confidence interval (CI) 0.62−1.60), p = 0.98, heterogeneity (I2) 43%], MI [5.3% vs. 5.9%, RR: 0.93 (95%CI 0.66−1.32), p = 0.69, I2 42%], or unplanned revascularisation [7.4% vs. 7.9%, RR: 0.92 (95%CI 0.76−1.11), p = 0.37, I2 0%]. However, the number patients undergoing planned revascularisation by either stent or surgery was significantly lower with an FFR-guided strategy [weighted mean difference: 14 (95% CI 3 to 25)%, p =< 0.001]. Conclusion: In patients with obstructive CAD, an FFR-guided management strategy did not impact on all-cause mortality, MI and unplanned revascularisation, when compared to an angiography-guided management strategy, but led to up to a quarter less patients needing revascularisation.
比较血流储备分数(FFR)指导与血管造影指导下治疗阻塞性冠状动脉疾病(CAD)的随机对照试验(RCT)结果相互矛盾。我们研究了FFR指导与血管造影指导的治疗策略在阻塞性CAD患者中的疗效和安全性。方法:对主要数据库进行从创建到2022年9月的系统电子检索。我们纳入了出现心绞痛或心肌梗死(MI)、接受药物治疗、经皮冠状动脉介入治疗或搭桥手术的患者研究。采用随机效应模型合并风险比(RR)进行荟萃分析。感兴趣的终点是全因死亡率、MI和非计划血管重建。结果:纳入8项RCT,5077例患者有结局数据。加权平均随访时间为22个月。将FFR指导的治疗与血管造影指导的治疗进行比较时,全因死亡率[3.5%对3.7%,RR:0.99(95%置信区间(CI)0.62−1.60),p = 0.98,异质性(I²)43%]、MI[5.3%对5.9%,RR:0.93(95%CI 0.66−1.32),p = 0.69,I² 42%]或非计划血管重建[7.4%对7.9%,RR:0.92(95%CI 0.76−1.11),p = 0.37,I² 0%]无差异。然而,采用FFR指导策略时,通过支架或手术进行计划血管重建的患者数量显著减少[加权平均差异:14(95%CI 3至25)%,p <= 0.001]。结论:在阻塞性CAD患者中,与血管造影指导的治疗策略相比,FFR指导的治疗策略对全因死亡率、MI和非计划血管重建无影响,但需要血管重建的患者减少了多达四分之一。