Sandau Charlotte, Hansen Ejvind Frausing, Pedersen Lars, Jensen Jens Ulrik Stæhr
Department of Respiratory Medicine and Endocrinology, Pulmonary Section, Copenhagen University Hospital Hvidovre, Copenhagen, Denmark.
Department of Respiratory Medicine and Infectious Diseases, Copenhagen Univervisity Hospital Bispebjerg Hospital, Copenhagen, Denmark.
Eur Clin Respir J. 2022 Dec 5;10(1):2153644. doi: 10.1080/20018525.2022.2153644. eCollection 2023.
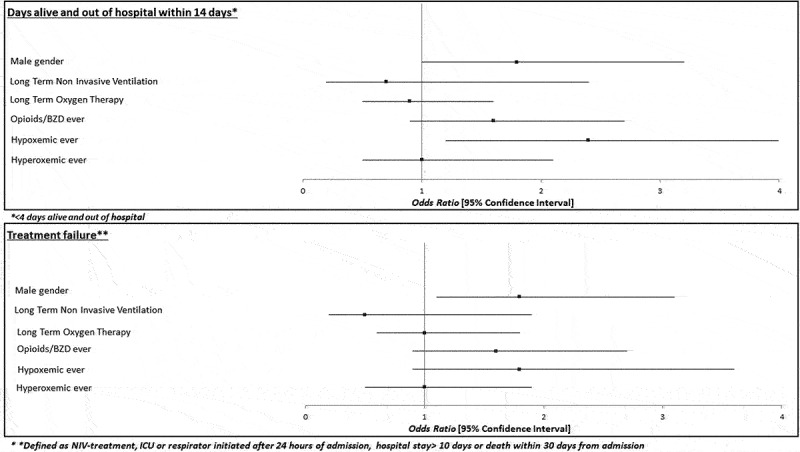
For patients admitted with an acute exacerbation of COPD (AECOPD) and a need for supplementary oxygen therapy, to determine if peripheral oxygen saturation < 88% (hypoxemia) or >92% (hyperoxemia), within first 24 hours of admission, is associated with 'treatment failure' or fewer days alive and out of hospital within 14 days after admission.
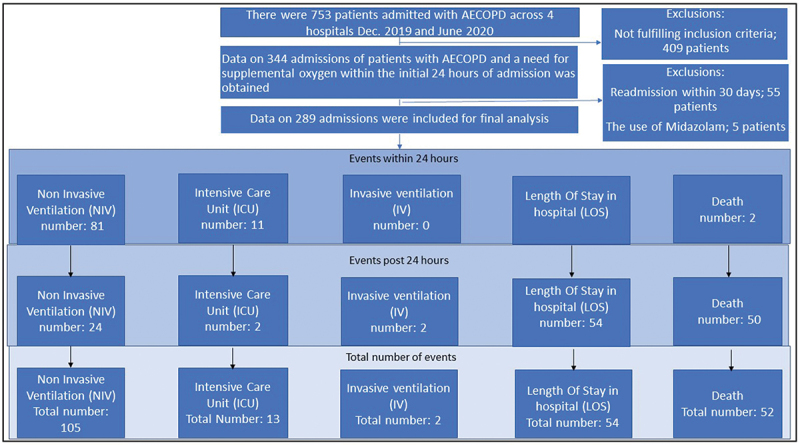
A retrospective multicenter observational study, reviewing consecutive data on SpO2, oxygen, and drug administration at three predefined time points, on adverse events in patients admitted with COPD between December 2019 and June 2020. Multivariable logistic regression analysis, Mann Whitney U- and Chi-square-test were used.
Acute hospital setting, across four different hospitals in the capital region of Denmark.
Patients with a confirmed diagnosis of COPD admitted with an acute exacerbation and an oxygen need within the first 24 hours admission.
In total 289 COPD patients were included. The median age was 74.8 years [interquartile range (IQR):69.6 to 81.8], 191 were female and 132 patients experienced 'treatment failure'. A minimum of one episode of hypoxemia (SpO < 88%) within first 24 hours was associated with having a low number (≤4) of days alive and out of hospital within 14 days after admission: OR 2.4 (95%CI 1.2 to 4.8), p = 0.02, absolute risk 44% vs. 26% p = 0.01, Chi-square. Comparable results were observed after 30 days of follow-up: OR 2.6 (95% CI 1.0 to7.1), p = 0.05. A minimum of one measurement of hyperoxemia (SpO > 92%), within first 24 hours of admission was not associated with low number of days alive and out of hospital within 14 days OR 1.0 (95% CI 0.5 to 2.1) nor at 30 days.
For admitted patients with AECOPD, being hypoxemic ever within the first 24 hours after admission is associated with a substantially increased risk of a poor prognosis.
对于因慢性阻塞性肺疾病急性加重(AECOPD)入院且需要补充氧气治疗的患者,确定入院后24小时内外周血氧饱和度<88%(低氧血症)或>92%(高氧血症)是否与“治疗失败”或入院后14天内存活且出院天数减少有关。
一项回顾性多中心观察性研究,回顾了2019年12月至2020年6月期间因慢性阻塞性肺疾病入院患者在三个预定义时间点的连续血氧饱和度、氧气和药物给药数据以及不良事件。采用多变量逻辑回归分析、曼-惠特尼U检验和卡方检验。
丹麦首都地区四家不同医院的急性医院环境。
确诊为慢性阻塞性肺疾病且在入院后24小时内因急性加重需要吸氧的患者。
共纳入289例慢性阻塞性肺疾病患者。中位年龄为74.8岁[四分位间距(IQR):69.6至81.8],191例为女性,132例患者出现“治疗失败”。入院后24小时内至少有一次低氧血症发作(SpO<88%)与入院后14天内存活且出院天数少(≤4天)相关:比值比2.4(95%置信区间1.2至4.8),p = 0.02,绝对风险44%对26%,p = 0.01,卡方检验。随访30天后观察到类似结果:比值比2.6(95%置信区间1.0至7.1),p = 0.05。入院后24小时内至少有一次高氧血症测量值(SpO>92%)与14天内或30天内存活且出院天数少无关,比值比1.0(95%置信区间0.5至2.1)。
对于因AECOPD入院的患者,入院后24小时内出现低氧血症与预后不良风险大幅增加相关。