Bots Sophie H, Riera-Arnau Judit, Belitser Svetlana V, Messina Davide, Aragón Maria, Alsina Ema, Douglas Ian J, Durán Carlos E, García-Poza Patricia, Gini Rosa, Herings Ron M C, Huerta Consuelo, Sisay Malede Mequanent, Martín-Pérez Mar, Martin Ivonne, Overbeek Jetty A, Paoletti Olga, Pallejà-Millán Meritxell, Schultze Anna, Souverein Patrick, Swart Karin M A, Villalobos Felipe, Klungel Olaf H, Sturkenboom Miriam C J M
Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, Utrecht University, Utrecht, Netherlands.
Department of Datascience and Biostatistics, Julius Center for Health Sciences and Primary Health, University Medical Center Utrecht, Utrecht, Netherlands.
Front Pharmacol. 2022 Nov 24;13:1038043. doi: 10.3389/fphar.2022.1038043. eCollection 2022.
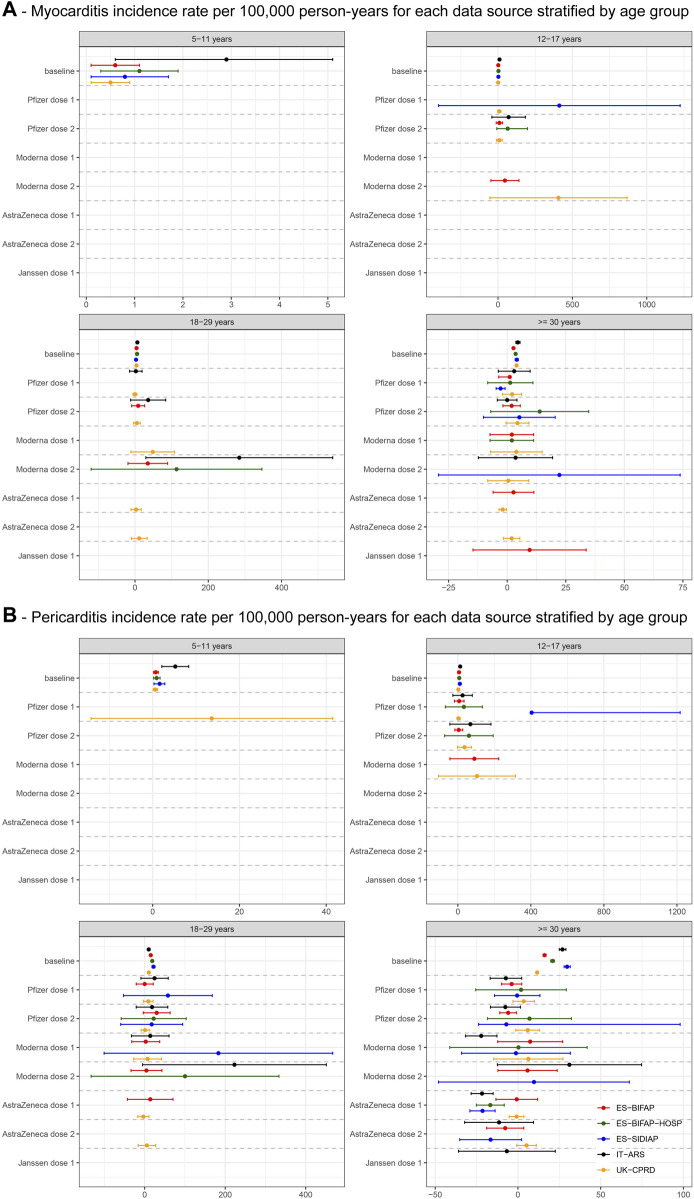
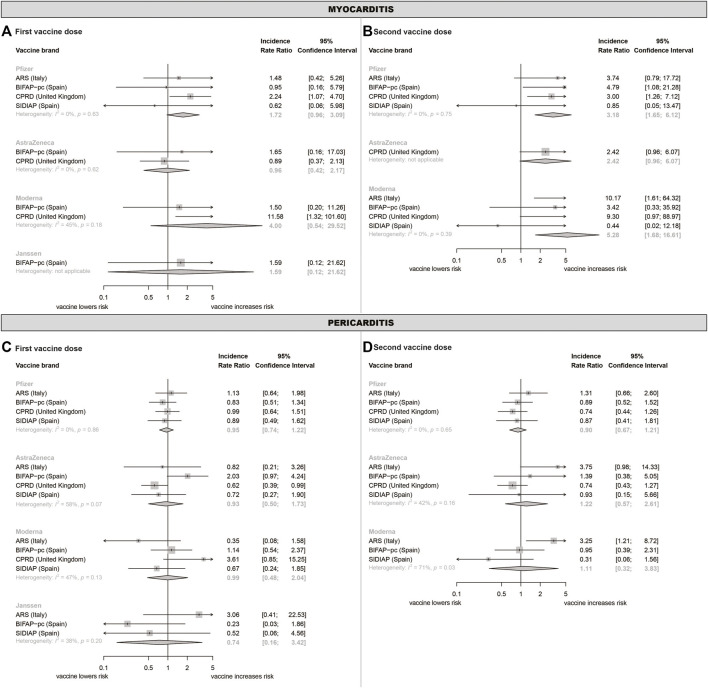
Estimates of the association between COVID-19 vaccines and myo-/pericarditis risk vary widely across studies due to scarcity of events, especially in age- and sex-stratified analyses. Population-based cohort study with nested self-controlled risk interval (SCRI) using healthcare data from five European databases. Individuals were followed from 01/01/2020 until end of data availability (31/12/2021 latest). Outcome was first myo-/pericarditis diagnosis. Exposures were first and second dose of Pfizer, AstraZeneca, Moderna, and Janssen COVID-19 vaccines. Baseline incidence rates (IRs), and vaccine- and dose-specific IRs and rate differences were calculated from the cohort The SCRI calculated calendar time-adjusted IR ratios (IRR), using a 60-day pre-vaccination control period and dose-specific 28-day risk windows. IRRs were pooled using random effects meta-analysis. Over 35 million individuals (49·2% women, median age 39-49 years) were included, of which 57·4% received at least one COVID-19 vaccine dose. Baseline incidence of myocarditis was low. Myocarditis IRRs were elevated after vaccination in those aged < 30 years, after both Pfizer vaccine doses (IRR = 3·3, 95%CI 1·2-9.4; 7·8, 95%CI 2·6-23·5, respectively) and Moderna vaccine dose 2 (IRR = 6·1, 95%CI 1·1-33·5). An effect of AstraZeneca vaccine dose 2 could not be excluded (IRR = 2·42, 95%CI 0·96-6·07). Pericarditis was not associated with vaccination. mRNA-based COVID-19 vaccines and potentially AstraZeneca are associated with increased myocarditis risk in younger individuals, although absolute incidence remains low. More data on children (≤ 11 years) are needed.
由于事件数量稀少,尤其是在年龄和性别分层分析中,关于新冠疫苗与心肌炎/心包炎风险之间关联的估计在不同研究中差异很大。基于人群的队列研究,采用嵌套自我对照风险区间(SCRI),使用来自五个欧洲数据库的医疗数据。个体从2020年1月1日开始随访,直至数据可用结束(最晚至2021年12月31日)。结局为首次心肌炎/心包炎诊断。暴露因素为辉瑞、阿斯利康、莫德纳和杨森新冠疫苗的第一剂和第二剂。从队列中计算基线发病率(IRs)以及疫苗和剂量特异性IRs和率差。SCRI使用接种前60天的对照期和剂量特异性28天风险窗口计算日历时间调整后的IR比值(IRR)。使用随机效应荟萃分析对IRR进行汇总。纳入了超过3500万人(49.2%为女性,中位年龄39 - 49岁),其中57.4%接受了至少一剂新冠疫苗。心肌炎的基线发病率较低。在年龄<30岁的人群中,接种疫苗后心肌炎IRR升高,辉瑞疫苗两剂后(IRR分别为3.3,95%CI 1.2 - 9.4;7.8,95%CI 2.6 - 23.5)以及莫德纳疫苗第二剂后(IRR = 6.1,95%CI 1.1 - 33.5)。不能排除阿斯利康疫苗第二剂的影响(IRR = 2.42,95%CI 0.96 - 6.07)。心包炎与接种疫苗无关。基于mRNA的新冠疫苗以及可能的阿斯利康疫苗与年轻个体中心肌炎风险增加相关,尽管绝对发病率仍然较低。需要更多关于儿童(≤11岁)的数据。