Malaithong Wanwipha, Tontisirin Nuj, Seangrung Rattaphol, Wongsak Siwadol, Cohen Steven P
Department of Anesthesiology, Phramongkutklao Hospital, Bangkok, Thailand.
Department of Anesthesiology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Reg Anesth Pain Med. 2022 Dec 21;48(4):151-60. doi: 10.1136/rapm-2022-103976.
Variability in anatomy in the knees supports the use of aggressive lesioning techniques such as bipolar-radiofrequency ablation (RFA) to treat knee osteoarthritis (KOA). There are no randomized controlled trials evaluating the efficacy of bipolar-RFA.
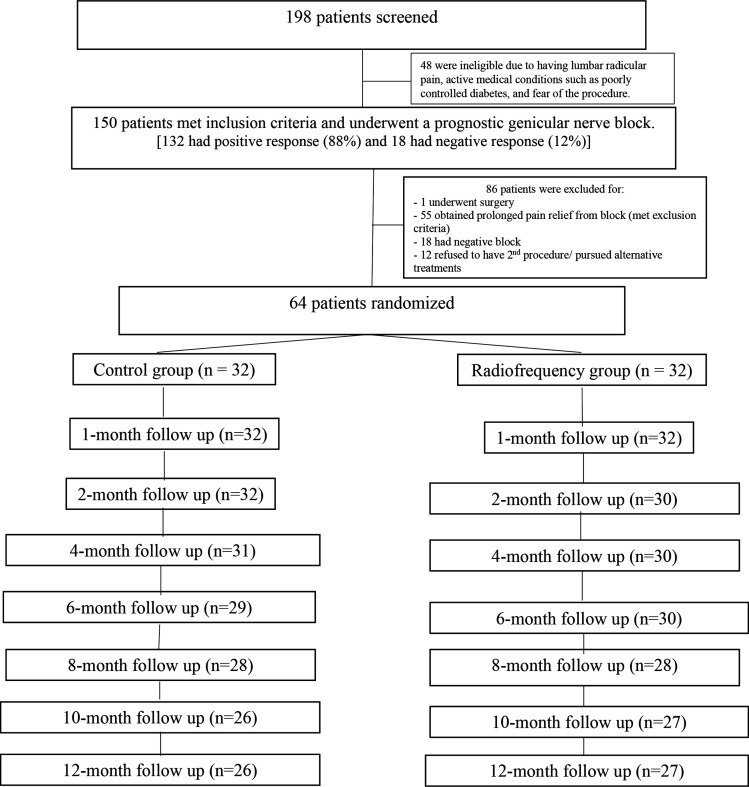
Sixty-four patients with KOA who experienced >50% pain relief from prognostic superomedial, superolateral and inferomedial genicular nerve blocks were randomly assigned to receive either genicular nerve local anesthetic and steroid injections with sham-RFA or local anesthetic and steroid plus bipolar-RFA. Participants and outcome adjudicators were blinded to allocation. The primary outcome was Visual Analog Scale pain score 12 months postprocedure. Secondary outcome measures included Western Ontario and McMaster Universities Arthritis (WOMAC) and Patient Global Improvement-Indexes (PGI-I).
Both groups experienced significant reductions in pain, with no significant differences observed at 12 months (reduction from 5.7±1.9 to 3.2±2.6 in the RFA-group vs from 5.0±1.4 to 2.6±2.4 in the control-group (p=0.40)) or any other time point. No significant changes were observed between groups for WOMAC and PGI-I at the primary endpoint, with only the control group experiencing a significant improvement in function at 12-month follow-up (mean reduction from 91.2±38.2 to 67.1±51.9 in the RFA-group (p=0.06) vs from 95.8±41.1 to 60.6±42.8 in the control group (p=0.001); p=0.85 between groups).
Our failure to find efficacy for genicular nerve RFA, coupled with evidence showing that a plenitude of nerves supply the knee joint and preliminary studies indicating superiority of lesioning strategies targeting more than three nerves, suggest controlled trials using more aggressive lesioning strategies are warranted.
TCTR20170130003.
膝关节解剖结构的变异性支持采用双极射频消融术(RFA)等积极的损伤技术来治疗膝关节骨关节炎(KOA)。目前尚无评估双极RFA疗效的随机对照试验。
64例经预后性膝上内侧、膝上外侧和膝下内侧神经阻滞疼痛缓解超过50%的KOA患者,被随机分配接受膝关节神经局部麻醉药和类固醇注射加假RFA或局部麻醉药和类固醇加双极RFA。参与者和结果判定者对分组情况不知情。主要结局是术后12个月的视觉模拟量表疼痛评分。次要结局指标包括西安大略和麦克马斯特大学骨关节炎指数(WOMAC)和患者总体改善指数(PGI-I)。
两组患者的疼痛均显著减轻,在12个月时(RFA组从5.7±1.9降至3.2±2.6,对照组从5.0±1.4降至2.6±2.4,p = 0.40)或任何其他时间点均未观察到显著差异。在主要终点时,两组的WOMAC和PGI-I均未观察到显著变化,仅对照组在12个月随访时功能有显著改善(RFA组从91.2±38.2降至67.1±51.9,p = 0.06;对照组从95.8±41.1降至60.6±42.8,p = 0.001;组间p = 0.85)。
我们未能发现膝关节神经RFA的疗效,再加上有证据表明膝关节由大量神经支配,以及初步研究表明针对三条以上神经的损伤策略具有优越性,这表明有必要进行采用更积极损伤策略的对照试验。
TCTR20170130003。