Department of Neurology, Massachusetts General Hospital, Boston (L.M.V.R.M., M.A.D., Z.Y., L.H.S.).
Department of Neurology, Harvard Medical School, Boston, MA (L.M.V.R.M., L.H.S.).
Stroke. 2023 Feb;54(2):527-536. doi: 10.1161/STROKEAHA.122.039946. Epub 2022 Dec 21.
Older adults occasionally receive seizure prophylaxis in an acute ischemic stroke (AIS) setting, despite safety concerns. There are no trial data available about the net impact of early seizure prophylaxis on post-AIS survival.
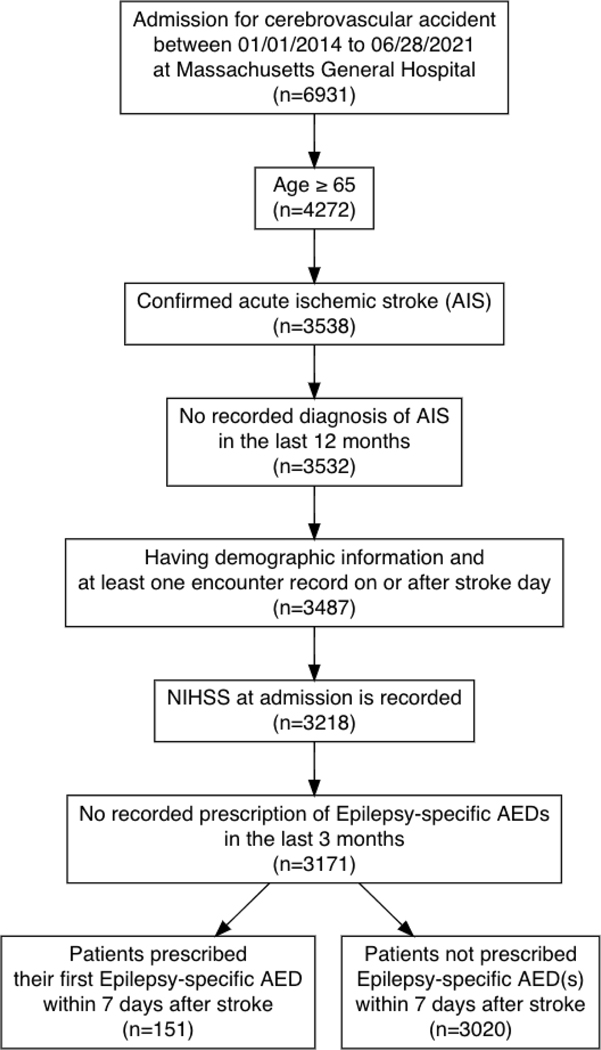
Using a stroke registry (American Heart Association's Get With The Guidelines) individually linked to electronic health records, we examined the effect of initiating seizure prophylaxis (ie, epilepsy-specific antiseizure drugs) within 7 days of an AIS admission versus not initiating in patients ≥65 years admitted for a new, nonsevere AIS (National Institutes of Health Stroke Severity score ≤20) between 2014 and 2021 with no recorded use of epilepsy-specific antiseizure drugs in the previous 3 months. We addressed confounding by using inverse-probability weights. We performed standardization accounting for pertinent clinical and health care factors (eg, National Institutes of Health Stroke Severity scale, prescription counts, seizure-like events).
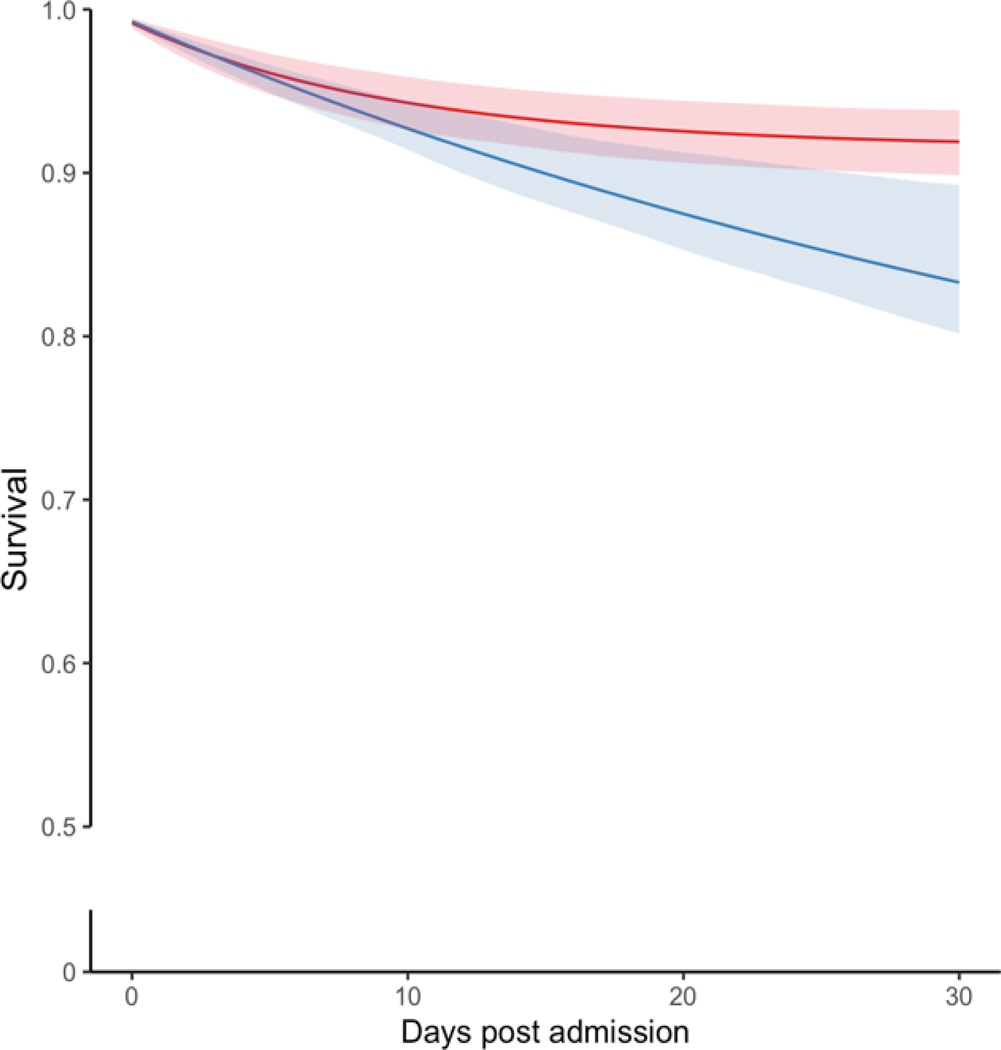
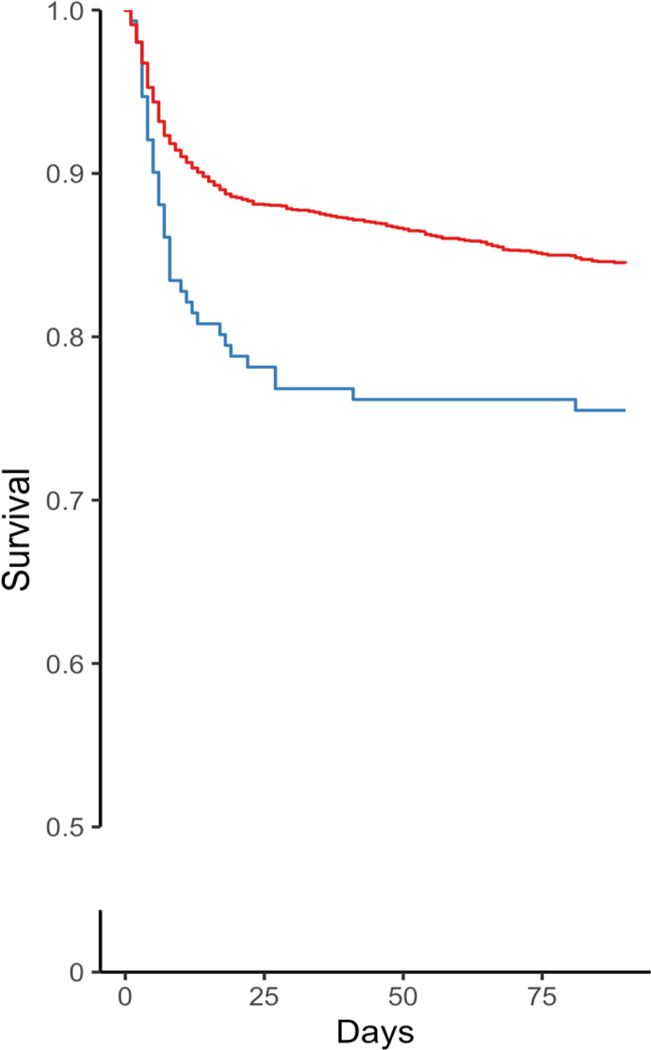
The study sample included 151 patients who received antiseizure drugs and 3020 who did not. The crude 30-day mortality risks were 219 deaths per 1000 patients among epilepsy-specific antiseizure drugs initiators and 120 deaths per 1000 among noninitiators. After standardization, the estimated mortality was 251 (95% CI, 190-307) deaths per 1000 among initiators and 120 (95% CI, 86-144) deaths per 1000 among noninitiators, corresponding to a risk difference of 131 (95% CI, 65-200) excess deaths per 1000 patients. In the prespecified subgroup analyses, the risk difference was 52 (95% CI, 11-72) among patients with minor AIS and 138 (95% CI, 52-222) among moderate-to-severe AIS patients. Similarly, the risk differences were 86 (95% CI, 18-118) and 157 (95% CI, 57-219) among patients aged 65 to 74 years and ≥75 years, respectively.
There was a higher risk of 30-day mortality associated with initiating versus not initiating seizure prophylaxis within 7 days post-AIS. This study does not support the role of seizure prophylaxis in reducing 30-day poststroke mortality.
尽管存在安全性问题,老年人在急性缺血性脑卒中(AIS)发生时偶尔会接受预防性抗癫痫治疗。目前尚无关于早期预防性抗癫痫治疗对 AIS 后生存的净影响的临床试验数据。
我们使用一个卒中登记库(美国心脏协会的 Get With The Guidelines),该登记库与电子病历单独关联,对 2014 年至 2021 年期间新诊断为非严重 AIS(美国国立卫生研究院卒中严重程度评分≤20)且在过去 3 个月内未使用过癫痫特异性抗癫痫药物的年龄≥65 岁的患者进行了研究,这些患者在 AIS 入院后 7 天内开始预防性抗癫痫治疗(即,使用癫痫特异性抗癫痫药物)与未开始治疗进行了比较。我们通过使用逆概率权重来解决混杂因素。我们进行了标准化处理,考虑了相关的临床和医疗保健因素(例如,美国国立卫生研究院卒中严重程度量表、处方数量、癫痫样事件)。
本研究样本包括 151 例接受抗癫痫药物治疗的患者和 3020 例未接受治疗的患者。癫痫特异性抗癫痫药物治疗组的 30 天死亡率为每 1000 例患者 219 例死亡,而非治疗组为每 1000 例患者 120 例死亡。标准化后,治疗组估计死亡率为每 1000 例患者 251 例(95%CI,190-307),而非治疗组为每 1000 例患者 120 例(95%CI,86-144),相应的风险差异为每 1000 例患者 131 例(95%CI,65-200)超额死亡。在预先指定的亚组分析中,轻度 AIS 患者的风险差异为 52 例(95%CI,11-72),中度至重度 AIS 患者的风险差异为 138 例(95%CI,52-222)。同样,65-74 岁和≥75 岁患者的风险差异分别为 86 例(95%CI,18-118)和 157 例(95%CI,57-219)。
与 AIS 后 7 天内不开始预防性抗癫痫治疗相比,开始治疗与 30 天内死亡率升高相关。本研究不支持预防性抗癫痫治疗在降低卒中后 30 天死亡率方面的作用。