Barnabee Gena, O'Bryan Gillian, Ndeikemona Lylie, Billah Idel, Silas Lukas, Morgan Karie L, Shulock Katherine, Mawire Susan, MacLachlan Ellen, Nghipangelwa Josua, Muremi Elizabeth, Ensminger Alison, Forster Norbert, O'Malley Gabrielle
International Training and Education Center for Health, Department of Global Health, University of Washington, Seattle, WA, United States.
Directorate of Special Programmes, Ministry of Health and Social Services, Windhoek, Namibia.
Front Reprod Health. 2022 Dec 5;4:1048702. doi: 10.3389/frph.2022.1048702. eCollection 2022.
Despite the potential for community-based approaches to increase access to pre-exposure prophylaxis (PrEP) for adolescent girls and young women (AGYW), there is limited evidence of whether and how they improve PrEP persistence. We compared PrEP persistence among AGYW receiving services through community and hybrid models in Namibia to facility-based services. We subsequently identify potential mechanisms to explain how and why community and hybrid models achieved (or not) improved persistence to inform further service delivery innovation.
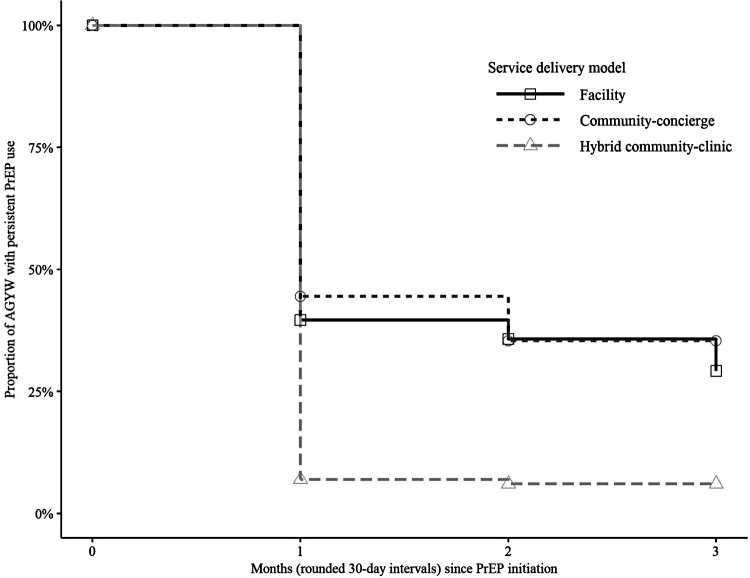
Data were collected from PrEP service delivery to AGYW over two-years in Namibia's Khomas Region. We used Kaplan-Meier analysis to estimate survival curves for PrEP persistence beyond three-months after initiation and report the cumulative probability of persistence at one- and three-months. Persistence was defined as any PrEP use within three months after initiation followed by a PrEP refill or previously prescribed supply of at least 30 days at the three-month visit. Interviews were conducted with 28 AGYW and 19 providers and analyzed using a deductive-inductive thematic approach.
From October 2017 through September 2019, 372 (18.7%) AGYW received services through a facility model, 302 (15.1%) through a community model, and 1,320 (66.2%) through a hybrid model. PrEP persistence at one- and three-months was 41.2% and 34.9% in the community model and 6.2% and 4.8% in the hybrid model compared to 36.8% and 26.7% in the facility model. Within the community and hybrid models, we identified three potential mechanisms related to PrEP persistence. Individualized service delivery offered which enabled AGYW to overcome barriers to obtaining refills but did not work as well for highly mobile AGYW. Consistent interactions and shared experiences fostered , building social networks and support systems for PrEP use. PrEP and HIV-related stigma, however, was widely experienced outside of these networks. Community-to-facility referral for PrEP refill triggered in AGYW, which discouraged persistence.
Service delivery approaches that offer convenience and simplicity and foster social connectedness may reduce access barriers and increase social support enabling AGYW to self-manage their PrEP use and achieve improved PrEP persistence.
尽管基于社区的方法有可能增加少女和年轻女性(AGYW)获得暴露前预防(PrEP)的机会,但关于这些方法是否以及如何提高PrEP持续性的证据有限。我们比较了纳米比亚通过社区和混合模式接受服务的AGYW与基于机构的服务中PrEP的持续性。随后,我们确定了潜在机制,以解释社区和混合模式如何以及为何实现(或未实现)持续性的改善,为进一步的服务提供创新提供信息。
在纳米比亚霍马斯地区,收集了两年内为AGYW提供PrEP服务的数据。我们使用Kaplan-Meier分析来估计开始后三个月以上PrEP持续性的生存曲线,并报告在一个月和三个月时持续性的累积概率。持续性定义为开始后三个月内的任何PrEP使用,随后在三个月就诊时进行PrEP补充或先前开具的至少30天的供应量。对28名AGYW和19名提供者进行了访谈,并使用演绎-归纳主题方法进行了分析。
从2017年10月到2019年9月,372名(18.7%)AGYW通过机构模式接受服务,302名(15.1%)通过社区模式接受服务,1320名(66.2%)通过混合模式接受服务。社区模式中一个月和三个月时的PrEP持续性分别为41.2%和34.9%,混合模式中为6.2%和4.8%,而机构模式中为36.8%和26.7%。在社区和混合模式中,我们确定了与PrEP持续性相关的三个潜在机制。提供个性化服务交付,使AGYW能够克服获取补充剂的障碍,但对流动性高的AGYW效果不佳。持续的互动和共同的经历促进了PrEP的使用,建立了PrEP使用的社交网络和支持系统。然而,在这些网络之外,PrEP和与HIV相关的耻辱感普遍存在。社区到机构的PrEP补充剂转诊引发了AGYW的担忧,这不利于持续性。
提供便利和简单性并促进社会联系的服务提供方法可能会减少获取障碍并增加社会支持,使AGYW能够自我管理PrEP的使用并提高PrEP的持续性。