Ye Mengfan, Zhou Yun, Chen Huiru, Zhu Sijia, Diao Shanshan, Zhao Jieji, Kong Yan, Li Tan
Department of Neurology, The First Affiliated Hospital of Soochow University, No. 899, Pinghai Road, Suzhou 215006, China.
Brain Sci. 2022 Dec 6;12(12):1674. doi: 10.3390/brainsci12121674.
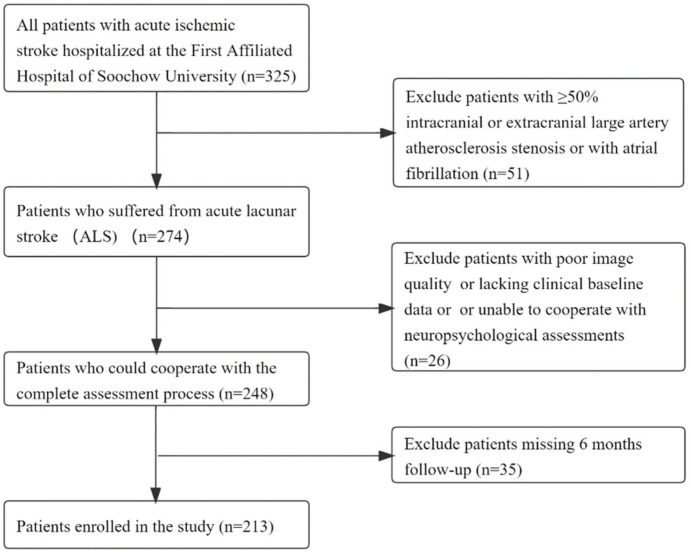
Background: The severity of white matter hyperintensity (WMH) in patients with acute lacunar stroke (ALS) may be not completely parallel to cognitive impairment. Controversies persist about the effects of WMH on cognitive dysfunction. It is vital to explore whether the association may be affected by certain factors and whether a subsequent subgroup analysis is necessary. The aim of this study was to evaluate the relationship between WMH and cognitive impairment in acute lacunar stroke patients and the possible causal factors. Methods: We continuously enrolled patients with ALS who were hospitalized at the First Affiliated Hospital of Soochow University between October 2017 and June 2022. The cognitive function of all patients was assessed by using the Montreal Cognitive Assessment (MoCA) scale 14 ± 2 days after the onset of AIS, and the results were adjusted to the education level. The MoCA scale was reevaluated at the 6-month (day 182 ± 7) follow-up by outpatient visit or video. Demographic and clinical data were collected. The manifestations of chronic cerebral small-vessel disease (CSVD), including the total Fazekas score and total CSVD burden score, were assessed with an MRI scan. A mismatch refers to an inconsistency between the severity of WMH and cognitive dysfunction. A Type 1 mismatch refers to cognitive impairment with mild WMH (total Fazekas score = 0−1), and a Type 2 mismatch refers to severe WMH (total Fazekas score = 5−6) in patients with normal cognitive function. Results: Among 213 enrolled ALS patients, 66 patients (31.0%) had cognitive dysfunction, and 40 patients (18.8%) had mismatches. Twenty-seven cases (12.7%) were Type 1 mismatched, and seventeen cases (8.0%) were Type 2 mismatched. Age, gender, fibrinogen and cerebral infarction history were independent risk factors for cognitive impairment in ALS patients. Imaging features, including moderate to severe WMH, deep WMH and the total CSVD burden score, were also independently associated with cognitive impairment. The patients in the mismatched group were older, had more severe deep WMH and had a higher occurrence of depression (p < 0.05). The NIHSS score, depression and microbleeds were significantly different between the Type 1 mismatched group and the matched group (p = 0.018, p = 0.012 and p = 0.047). Patients in the Type 2 mismatched group were male (p = 0.04), had a lower level of fibrinogen (p = 0.005), a lower incidence of CMBs (p = 0.003), a lower total CSVD burden score (p = 0.017), more severe paraventricular WMH (p = 0.035) and milder deep WMH (p = 0.026). Conclusions: Our study examined a homogeneous study cohort of recruited patients with symptomatic ALS. We found heterogeneity between WMH and cognitive function in ALS patients. Despite a similar WMH severity, some baseline clinical features and other conventional CSVD imaging characteristics may account for this heterogeneity phenomenon. Our findings provide data for the early diagnosis and prevention of cognitive impairment in ALS patients and suggest that the severity of WMH is not completely parallel to cognitive impairment. The white matter microstructural injury and remote WMH effects may account for the mismatch phenomenon. More attention should be paid to understanding the underlying mechanisms and finding new imaging markers.
急性腔隙性卒中(ALS)患者的白质高信号(WMH)严重程度可能与认知障碍并不完全平行。关于WMH对认知功能障碍的影响仍存在争议。探讨这种关联是否可能受到某些因素影响以及是否有必要进行后续亚组分析至关重要。本研究旨在评估急性腔隙性卒中患者中WMH与认知障碍之间的关系以及可能的因果因素。
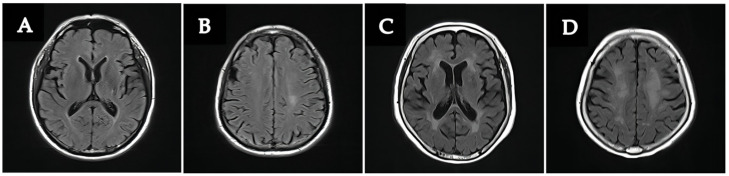
我们连续纳入了2017年10月至2022年6月期间在苏州大学附属第一医院住院的ALS患者。所有患者在急性缺血性卒中(AIS)发病后14±2天使用蒙特利尔认知评估(MoCA)量表评估认知功能,并根据教育水平进行结果调整。在6个月(第182±7天)随访时通过门诊就诊或视频方式再次评估MoCA量表。收集人口统计学和临床数据。通过MRI扫描评估慢性脑小血管病(CSVD)的表现,包括总 Fazekas评分和总CSVD负担评分。不匹配是指WMH严重程度与认知功能障碍之间的不一致。1型不匹配是指轻度WMH(总Fazekas评分=0-1)伴认知障碍,2型不匹配是指认知功能正常的患者中严重WMH(总Fazekas评分=5-6)。
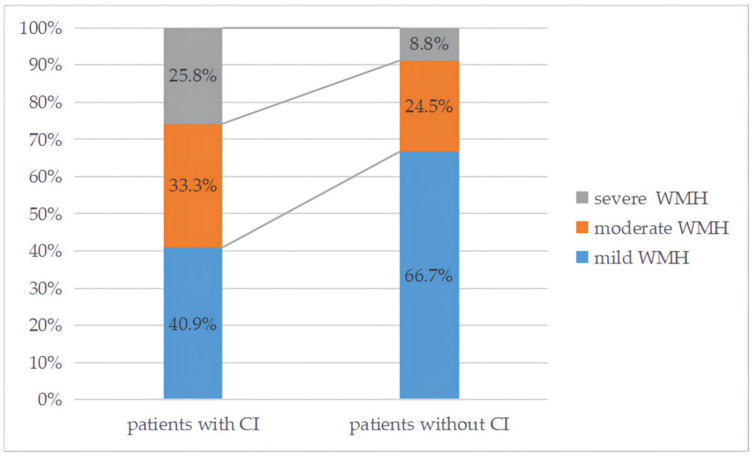
在213例纳入的ALS患者中,66例(31.0%)有认知功能障碍,40例(18.8%)存在不匹配情况。27例(12.7%)为1型不匹配,17例(8.0%)为2型不匹配。年龄、性别、纤维蛋白原和脑梗死病史是ALS患者认知障碍的独立危险因素。影像学特征,包括中度至重度WMH、深部WMH和总CSVD负担评分,也与认知障碍独立相关。不匹配组患者年龄更大,深部WMH更严重,抑郁症发生率更高(p<0.05)。1型不匹配组与匹配组之间的美国国立卫生研究院卒中量表(NIHSS)评分、抑郁症和微出血有显著差异(p=0.018、p=0.012和p=0.047)。2型不匹配组患者为男性(p=0.04),纤维蛋白原水平较低(p=0.005),CMBs发生率较低(p=0.003),总CSVD负担评分较低(p=0.017),脑室旁白质WMH更严重(p=0.035),深部WMH较轻(p=0.026)。
我们的研究检查了一组招募的有症状ALS患者的同质研究队列。我们发现ALS患者中WMH与认知功能之间存在异质性。尽管WMH严重程度相似,但一些基线临床特征和其他传统CSVD影像学特征可能解释了这种异质性现象。我们的研究结果为ALS患者认知障碍的早期诊断和预防提供了数据,并表明WMH严重程度与认知障碍并不完全平行。白质微结构损伤和远处WMH效应可能解释了不匹配现象。应更加关注理解潜在机制并寻找新的影像学标志物。