Department of Cardiology and Intensive Care Medicine, Asklepios Clinic St. Georg, Faculty of Medicine, Semmelweis University Campus Hamburg, 20099 Hamburg, Germany.
DZHK (German Center for Cardiovascular Research), Partner Site Hamburg/Kiel/Luebeck, 20251 Hamburg, Germany.
Medicina (Kaunas). 2022 Nov 22;58(12):1700. doi: 10.3390/medicina58121700.
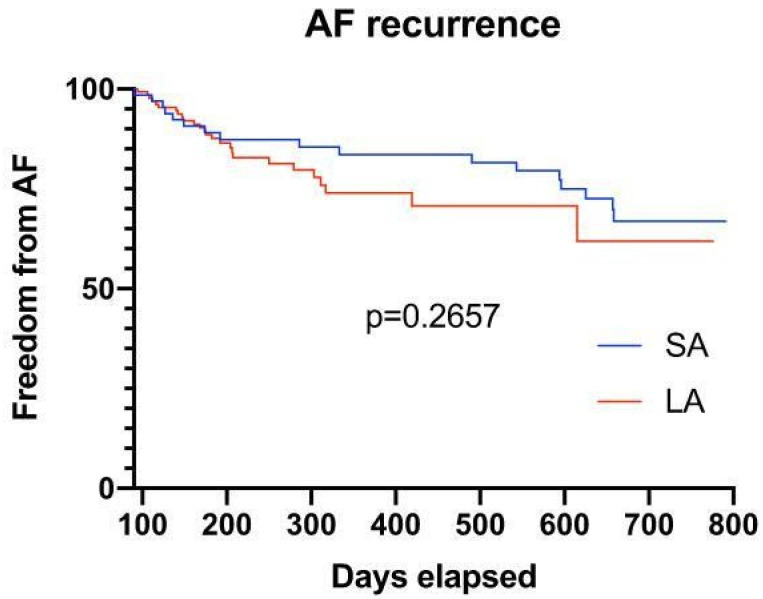
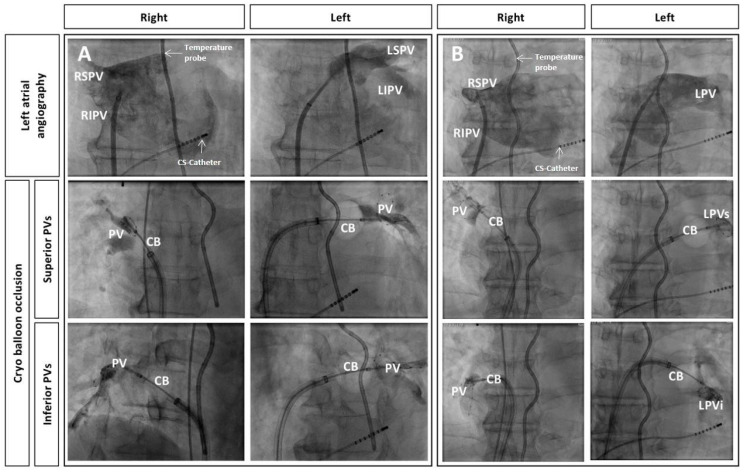
Background and Objectives: Selective pulmonary vein (PV) angiography has been established as the gold standard for PV visualization in cryoballoon (CB)-based pulmonary vein isolation (PVI). We sought to simplify this approach to reduce procedural complexity and radiation exposure. Materials and Methods: Patients with paroxysmal and recently diagnosed persistent AF undergoing CB-based PVI from January 2015 to December 2017 were retrospectively analyzed. Patients underwent either selective PV angiography or conventional left atrial (LA) angiography for PV visualization. Results: A total of 336 patients were analyzed. A total of 87 patients (26%) received PV angiography and 249 (74%) LA angiography. LA angiography required fewer cine-sequences for PV visualization, translating into a significant reduction in procedure duration, fluoroscopy time and dose area product. Additionally, less contrast medium was utilized. PV occlusion by the CB, CB temperature and time to isolation showed no significant differences. The number of CB applications and total application time (LA angiography: 1.4 ± 0.02 vs. PV Angiography: 1.6 ± 0.05; p < 0.0001; LA angiography: 297.9 ± 4.62 vs. PV-Angiography: 348.9 ± 11.03; p < 0.001, respectively) per vein were slightly but significantly higher in the PV angiography group. We observed no difference in late AF recurrence (24.7% LA angiography vs. 21.3% PV angiography; p = 0.2657). Conclusions: A simplified protocol, using LA angiography for PV visualization, entails a reduction in procedure time and radiation exposure while equally maintaining procedural efficiency and safety in both groups.
选择性肺静脉(PV)造影已被确立为冷冻球囊(CB)肺静脉隔离(PVI)中PV 可视化的金标准。我们旨在简化此方法,以减少操作复杂性和辐射暴露。材料与方法:回顾性分析了 2015 年 1 月至 2017 年 12 月期间接受 CB 基 PVI 的阵发性和近期诊断为持续性 AF 患者。患者接受选择性 PV 造影或常规左心房(LA)造影以显示 PV。结果:共分析了 336 例患者。共有 87 例(26%)患者接受了 PV 造影,249 例(74%)患者接受了 LA 造影。LA 造影术显示 PV 所需的电影序列更少,因此手术时间、透视时间和剂量面积乘积显著缩短。此外,造影剂用量也更少。CB 对 PV 的闭塞、CB 温度和隔离时间无显著差异。CB 的应用次数和总应用时间(LA 造影术:1.4±0.02 比 PV 造影术:1.6±0.05;p<0.0001;LA 造影术:297.9±4.62 比 PV 造影术:348.9±11.03;p<0.001)在 PV 造影组略有但有统计学意义地升高。我们发现两组之间晚期 AF 复发率无差异(LA 造影术:24.7%比 PV 造影术:21.3%;p=0.2657)。结论:使用 LA 造影术进行 PV 可视化的简化方案可减少手术时间和辐射暴露,同时在两组中保持相同的手术效率和安全性。