Gurung Anju, Poudel Dipesh, Gurung Bivek, Rawal Prabhat, Chapagain Sunder
Department of Internal Medicine, Nepal Armed Police Force Hospital, Kathmandu, NPL.
Department of Anaesthesiology, Nepal Armed Police Force Hospital, Kathmandu, NPL.
Cureus. 2022 Nov 24;14(11):e31866. doi: 10.7759/cureus.31866. eCollection 2022 Nov.
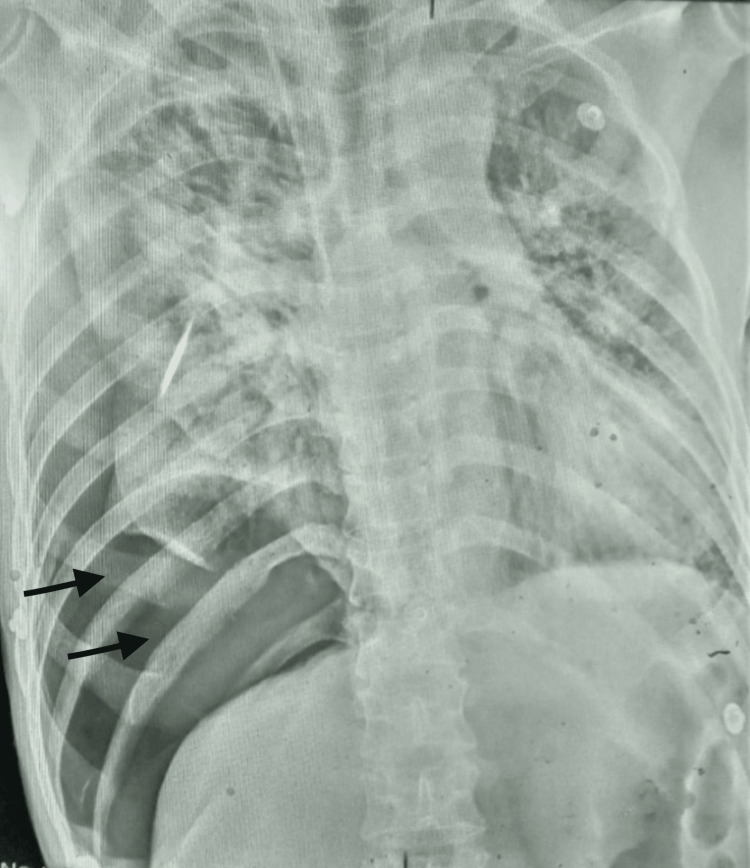
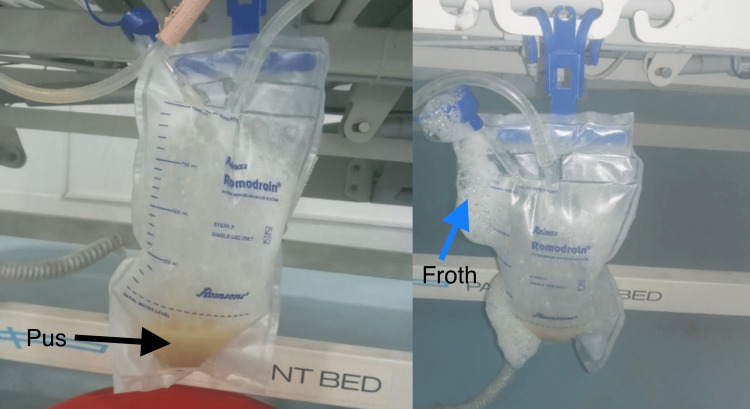
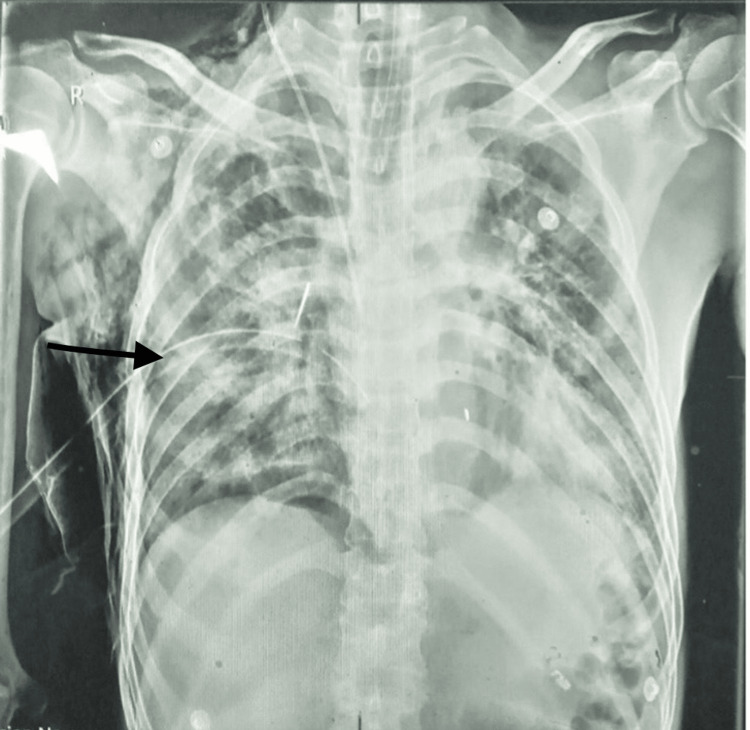
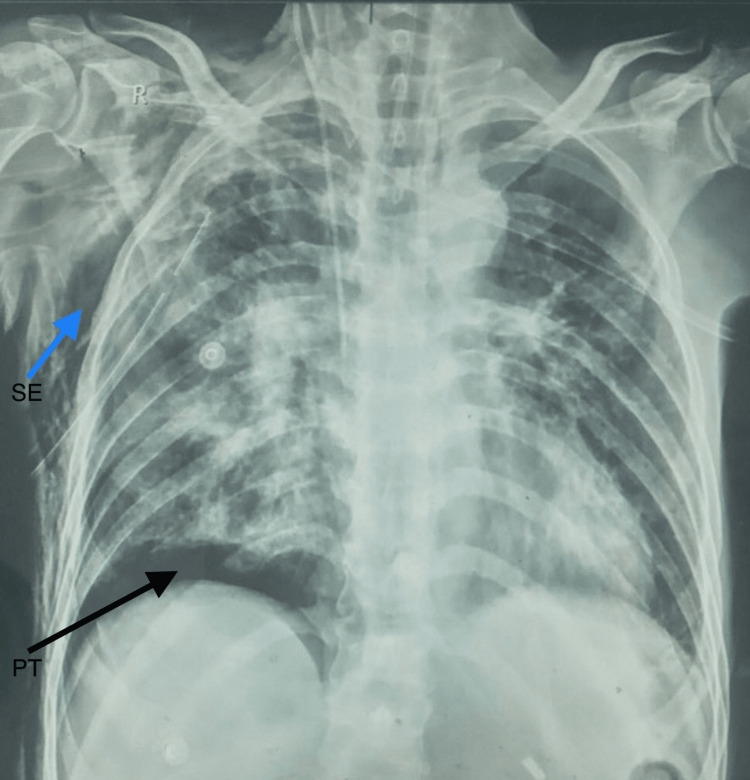
The COVID-19 pandemic has impacted every aspect of our lives since its start in December 2019. Among various COVID-19 complications, pleural complications are also increasingly reported but rarely from Nepal. Here, we presented a case of pyopneumothorax in a 52-year-old male patient referred from another center and admitted to the ICU of Nepal Armed Police Force Hospital with a diagnosis of severe COVID-19 pneumonia in the background of alcohol withdrawal syndrome with delirium tremens and generalized tonic-clonic seizures. He developed a rapid decline in respiratory status with a right-sided pneumothorax and underwent an immediate needle thoracostomy, followed by chest tube insertion. On the sixth day of admission, he had thick yellowish pus in the chest drain (pyopneumothorax), and despite the rigorous efforts in treatment, he died on the 15th day of admission. Though relatively uncommon, clinicians should consider pleural complications like pneumothorax, pleural effusion, pneumomediastinum, and empyema in patients with impaired immune status. In such patients, we should ensure prompt diagnosis with the earliest intervention and rationale use of antibiotics.
自2019年12月新冠疫情爆发以来,它已影响到我们生活的方方面面。在新冠病毒感染的各种并发症中,胸膜并发症的报道也越来越多,但在尼泊尔却很少见。在此,我们报告一例52岁男性患者的脓气胸病例,该患者从另一家中心转诊而来,因酒精戒断综合征伴震颤谵妄和全身强直阵挛性发作,以重症新冠病毒肺炎诊断入住尼泊尔武装警察部队医院重症监护病房。他因右侧气胸导致呼吸状况迅速恶化,随即接受了紧急胸腔穿刺术,随后插入胸腔引流管。入院第六天,胸腔引流管引出浓稠的黄色脓液(脓气胸),尽管进行了积极治疗,他仍在入院第15天死亡。虽然相对少见,但临床医生应考虑免疫功能受损患者出现的气胸、胸腔积液、纵隔气肿和脓胸等胸膜并发症。对于这类患者,我们应确保早期诊断并尽早干预,合理使用抗生素。