Spathoulas Konstantinos, Tsolaki Vasiliki, Zakynthinos George E, Karelas Dimitrios, Makris Demosthenes, Zakynthinos Epaminondas, Papanikolaou John
Department of Cardiology, General Hospital of Trikala, 42100 Trikala, Greece.
Department of Critical Care, School of Medicine, University of Thessaly, University Hospital of Larissa, 41110 Thessaly, Greece.
J Pers Med. 2022 Oct 29;12(11):1786. doi: 10.3390/jpm12111786.
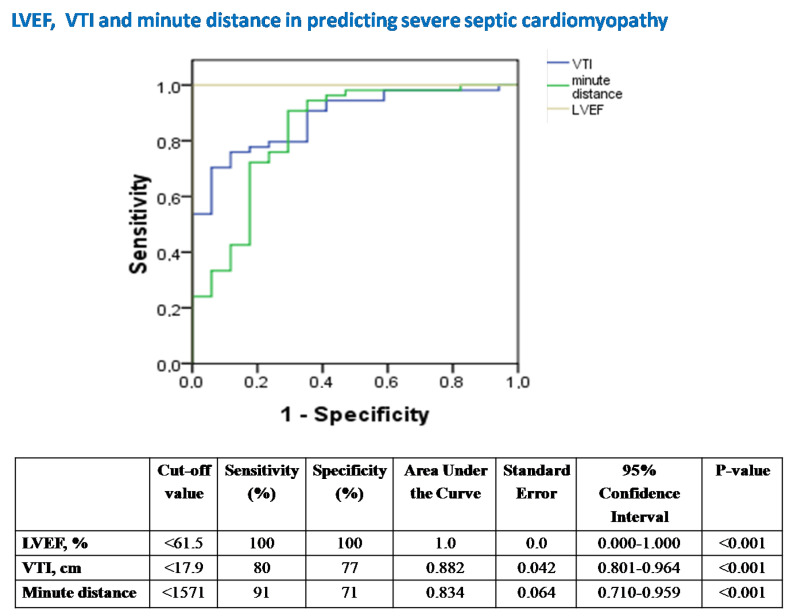
Background: the role of echocardiography in septic shock remains controversial, since depressed cardiac afterload may overestimate left ventricular (LV) systolic performance and mask septic cardiomyopathy (SC). We hypothesized that afterload-adjusted LV ejection fraction (LVEF) and LV outflow tract velocity-time integral (VTI) values for given systemic vascular resistances (SVR) could provide novel insights into recognizing and stratifying the severity of SC. Methods: in this observational, monocentric study, we prospectively included 14 mechanically-ventilated patients under septic-shock who all had a Pulse index Continuous Cardiac Output (PiCCO) system in place for hemodynamic monitoring. Echocardiographic and PiCCO longitudinal examinations (71 measurements overall) were performed simultaneously at the onset of septic shock and every 12 h for 60 h overall. Results: VTI-derived stroke volume (SV) and cardiac output (CO) were significantly correlated with PiCCO measurements (r ≥ 0.993, both p < 0.001). LVEF and VTI showed linear and exponential inverse correlation to SVR (R2 = 0.183 vs. 0.507 and p < 0.001 vs. p < 0.001, respectively). The equations LVEF = 86.168 − 0.011 × SVR and VTI = 41.23 × e(−0.0005×SVR) were found to provide “predicted” values for given SVR. Measured to predicted LVEF ratios (for given SVR), the afterload-adjusted LVEF defined the severity of SC (mild ≥ 90%, 80% ≤ moderate < 90% and severe < 80%). Mild SC demonstrated normal/supra-normal LVEF, normal VTI and SVR. Moderate SC showed lower LVEF and SVR, yet increased LV end-diastolic volume (LVEDV), VTI, SV and CO compared with mild SC (all p < 0.05). Severe SC was distinguished from moderate SC by markedly reduced LVEF, LVEDV, VTI, SV, CO and significantly increased SVR (all p < 0.05). LVEF and VTI decreased over time in mild SC, LVEF decreased in moderate SC, and LVEF and VTI increased over time in severe SC (p ≤ 0.038). LVEF and VTI demonstrated significant performance in identifying severe SC [cut-off < 61.5%, area under the curve (AUC) = 1 ± 0.0, sensitivity/specificity = 100/100, p < 0.001 vs. cut-off < 17.9 cm, AUC = 0.882 ± 0.042, sensitivity/specificity = 80/77, p < 0.001, respectively]. VTI but not LVEF demonstrated significant diagnostic performance in identifying both SVR < 800 dynes·s·cm−5 and SVR > 1500 dynes·s·cm−5 (cut-off > 24.46 cm, AUC = 0.889 ± 0.049, sensitivity/specificity = 75/100, p < 0.001; cut-off < 16.8, AUC = 0.0.857 ± 0.082, sensitivity/specificity = 83/86, p = 0.002, respectively).Conclusions: our study suggests that ICU bedside echocardiographic assessment of LVEF, VTI and their adjusted to corresponding SVR values provides valuable insights for the comprehension of SC phenotypes, underlying vasoplegia and cardiac output fluctuations in septic shock.
超声心动图在感染性休克中的作用仍存在争议,因为心脏后负荷降低可能高估左心室(LV)收缩功能并掩盖感染性心肌病(SC)。我们假设,对于给定的体循环血管阻力(SVR),经后负荷调整的左心室射血分数(LVEF)和左心室流出道速度时间积分(VTI)值可为识别和分层SC的严重程度提供新的见解。方法:在这项观察性单中心研究中,我们前瞻性纳入了14例感染性休克的机械通气患者,所有患者均安装了脉搏指示连续心输出量(PiCCO)系统进行血流动力学监测。在感染性休克发作时同时进行超声心动图和PiCCO纵向检查(共71次测量),并在60小时内每12小时进行一次。结果:VTI衍生的每搏输出量(SV)和心输出量(CO)与PiCCO测量值显著相关(r≥0.993,p均<0.001)。LVEF和VTI与SVR呈线性和指数负相关(R2分别为0.183和0.507,p分别<0.001和p<0.001)。发现方程LVEF = 86.168 - 0.011×SVR和VTI = 41.23×e(-0.0005×SVR)可为给定的SVR提供“预测”值。对于给定的SVR,经后负荷调整的LVEF根据测量值与预测值的比率定义了SC的严重程度(轻度≥90%,80%≤中度<90%,重度<80%)。轻度SC表现为正常/超正常LVEF、正常VTI和SVR。中度SC与轻度SC相比,LVEF和SVR较低,但左心室舒张末期容积(LVEDV)、VTI、SV和CO增加(所有p<0.05)。重度SC与中度SC的区别在于LVEF、LVEDV、VTI、SV、CO显著降低,SVR显著增加(所有p<0.05)。轻度SC中LVEF和VTI随时间下降,中度SC中LVEF下降,重度SC中LVEF和VTI随时间增加(p≤0.038)。LVEF和VTI在识别重度SC方面表现出显著性能[临界值<61.5%,曲线下面积(AUC)=1±0.0,敏感性/特异性=100/100,p<0.001;与临界值<17.9 cm相比,AUC = 0.882±0.042,敏感性/特异性=80/77,p<0.001]分别)。VTI而非LVEF在识别SVR<800达因·秒·厘米-5和SVR>1500达因·秒·厘米-5方面表现出显著诊断性能(临界值>24.46 cm,AUC = 0.889±0.049,敏感性/特异性=75/100,p<图0.001;临界值<16.8 cm,AUC = 0.857±0.082,敏感性/特异性=83/86,p = 0.002,分别)。结论:我们的研究表明,ICU床边超声心动图评估LVEF、VTI及其根据相应SVR值进行的调整,为理解感染性休克中的SC表型、潜在血管麻痹和心输出量波动提供了有价值的见解。