Lamarche-Fontaneto Raquel, Oud Lee, Howell Kayln D, Ganeriwal Simran A, Manek Gaurav U, Schleicher Mary C, Mallat Jihad, Cecconi Maurizio, Duggal Abhijit, Siuba Matthew T
Department of Pulmonary and Critical Care Medicine, Integrated Hospital Care Institute, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH, 44195, USA.
Department of Pulmonary and Critical Care Medicine, MedStar Southern Maryland Hospital Center, Clinton, MD, USA.
Crit Care. 2025 Jul 12;29(1):299. doi: 10.1186/s13054-025-05547-9.
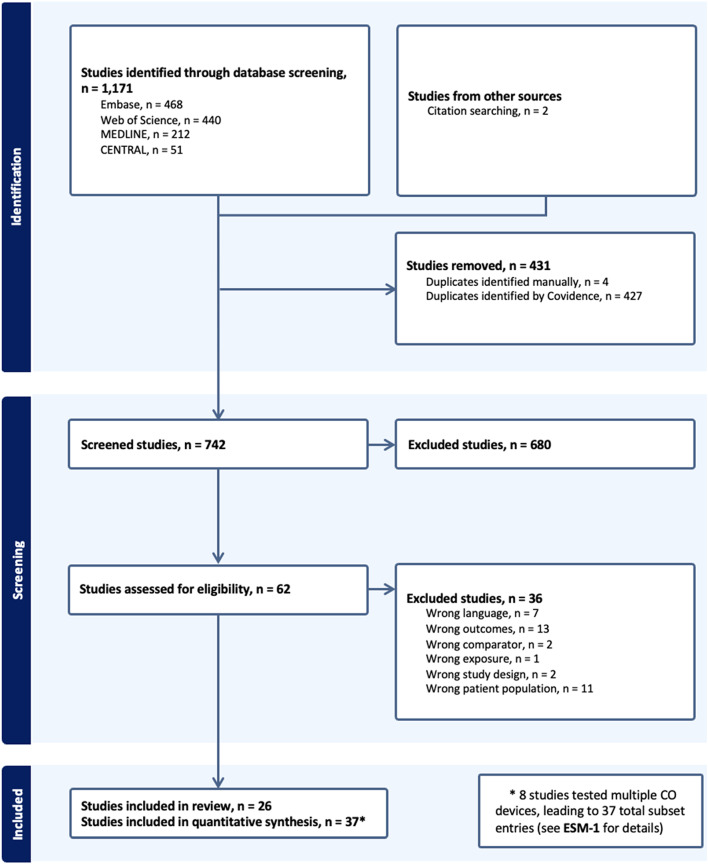
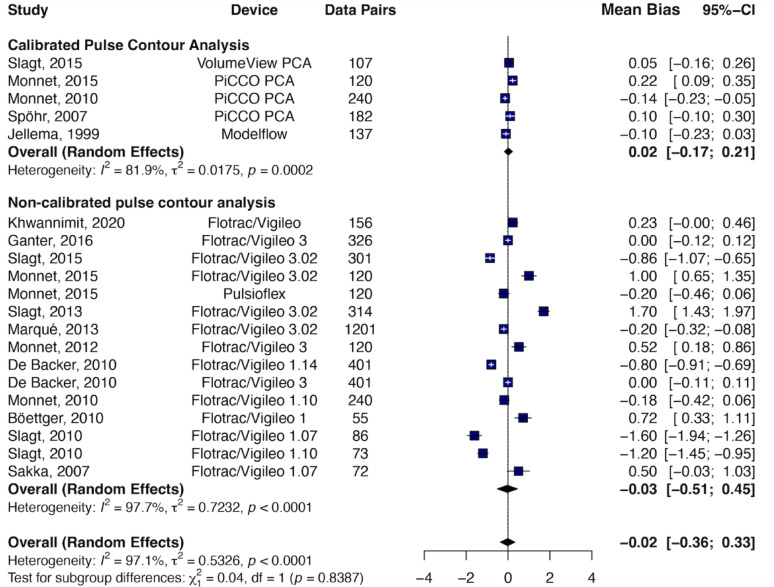
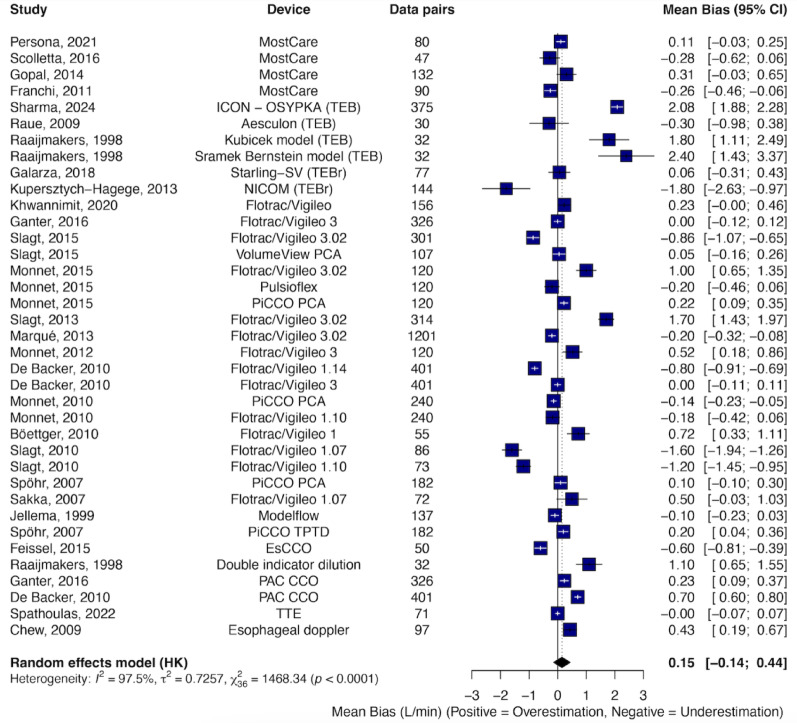
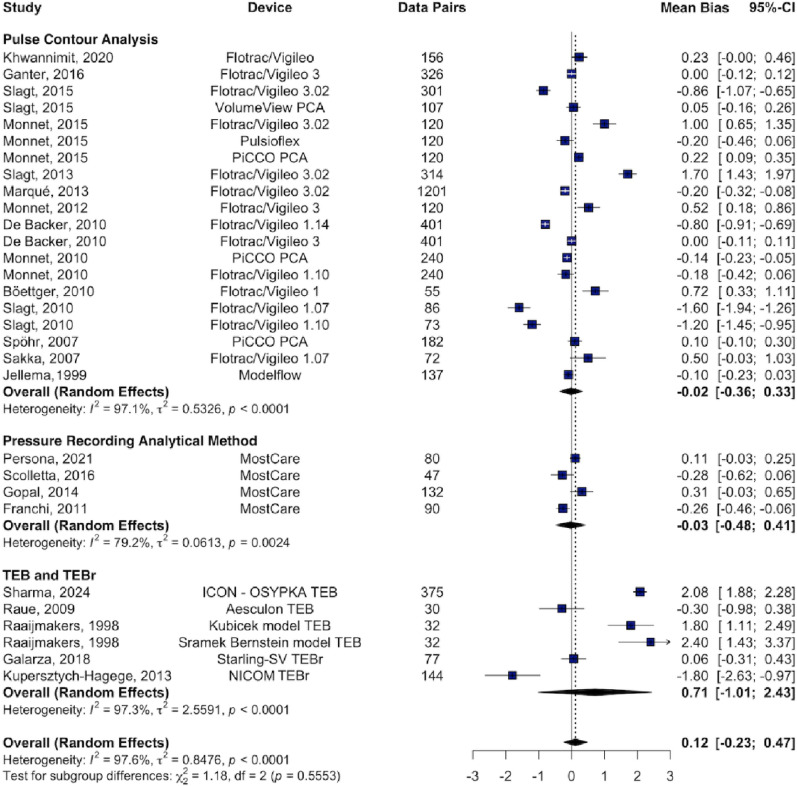
To evaluate the interchangeability of cardiac output (CO) monitoring devices compared to reference methods in adult ICU patients with septic shock, we systematically searched electronic databases through January 2025 for prospective studies comparing CO monitors with pulmonary artery catheter (PAC), transpulmonary thermodilution (TPTD), or echocardiography. Eligible studies included Bland-Altman analysis and, when available, trending assessment via polar or 4-quadrant plots, precision, and time response. Agreement was defined as percentage error (PE) < 30%, and acceptable trending as concordance ≥ 90%. Pooled bias, limits of agreement (LoA), and PE were calculated using the Sidik-Jonkman random-effects model. Twenty-six studies were included, yielding 37 unique device-reference datasets and encompassing 1,323 patients. PAC was the most common reference (18 datasets), followed by TPTD (16) and echocardiography (3). The pooled bias was 0.15 L min⁻¹ with LoA of ± 3.45 L min⁻¹ and pooled PE of 49%. Calibrated pulse contour analysis (PCA) showed the best agreement (PE 25%), whereas uncalibrated PCA, thoracic electrical bioimpedance, and bioreactance demonstrated poor agreement (PE ≥ 52%). Heterogeneity for mean bias was high across all subgroups (I² >80%). Of 15 datasets reporting trending, only three achieved concordance ≥ 90%. Most CO monitors demonstrate poor agreement with reference methods in septic shock. However, their true clinical utility remains unclear, as usual validation frameworks-centered on Bland-Altman analysis-overlook metrics that matter most to intensivists. Precision, time response, and trending ability are critical for real-time decision-making but were rarely assessed. Future studies must incorporate these parameters to meaningfully evaluate device performance at the bedside. PROSPERO registration: CRD42024509384.
为评估在患有脓毒性休克的成年重症监护病房患者中,心输出量(CO)监测设备与参考方法相比的互换性,我们系统检索了截至2025年1月的电子数据库,以查找比较CO监测仪与肺动脉导管(PAC)、经肺热稀释法(TPTD)或超声心动图的前瞻性研究。符合条件的研究包括Bland-Altman分析,以及在可行时通过极坐标图或四象限图进行的趋势评估、精密度和时间响应。一致性定义为百分比误差(PE)<30%,可接受的趋势定义为一致性≥90%。使用Sidik-Jonkman随机效应模型计算合并偏倚、一致性界限(LoA)和PE。纳入了26项研究,产生了37个独特的设备-参考数据集,涵盖1323名患者。PAC是最常用的参考方法(18个数据集),其次是TPTD(16个)和超声心动图(3个)。合并偏倚为0.15 L min⁻¹,LoA为±3.45 L min⁻¹,合并PE为49%。校准脉搏轮廓分析(PCA)显示出最佳一致性(PE 25%),而未校准的PCA、胸部电阻抗和生物反应性显示出较差的一致性(PE≥52%)。所有亚组的平均偏倚异质性都很高(I²>80%)。在报告趋势的15个数据集中,只有3个达到了一致性≥90%。大多数CO监测仪在脓毒性休克中与参考方法的一致性较差。然而,它们真正的临床效用仍不明确,因为以Bland-Altman分析为中心的常规验证框架忽略了对重症监护医生最重要的指标。精密度、时间响应和趋势能力对于实时决策至关重要,但很少被评估。未来的研究必须纳入这些参数,以便在床边有意义地评估设备性能。PROSPERO注册编号:CRD42024509384。