Department of Surgery Intensive Care Unit, China-Japan Friendship Hospital, Beijing, China.
Department of Emergency Medicine, China-Japan Friendship Hospital, Beijing, China.
J Appl Clin Med Phys. 2022 Aug;23(8):e13724. doi: 10.1002/acm2.13724. Epub 2022 Jul 11.
The application of point of care ultrasound (PoCUS) in medical education is a relatively new course. There are still great differences in the existence, quantity, provision, and depth of bedside ultrasound education. The left ventricular outflow tract velocity time integral (LVOT-VTI) has been successfully used in several studies as a parameter for hemodynamic management of critically ill patients, especially in the evaluation of fluid responsiveness. While LVOT-VTI has been broadly used, valuable applications using artificial intelligence (AI) in PoCUS is still limited. We aimed to identify the degree of correlation between auto LVOT-VTI and the manual LVOT-VTI acquired by PoCUS trained ICU doctors.
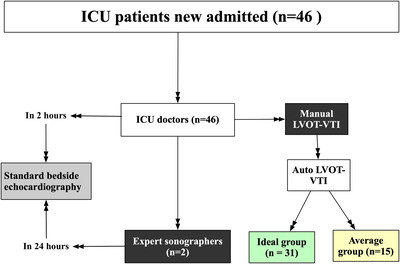
Among the 58 ICU doctors who attended PoCUS training from 1 September 2019 to 30 November 2020, 46 ICU doctors who trained for more than 3 months were enrolled. At the end of PoCUS training, each of the enrolled ICU doctors acquired echocardiography parameters of a new ICU patient in 2 h after new patient was admitted. One of the two bedside expert sonographers would take standard echocardiogram of new ICU patients within 24 h. For ICU doctors, manual LVOT-VTI was obtained for reference and auto LVOT-VTI was calculated instantly by using an AI software tool. Based on the image quality of the auto LVOT-VTI, ICU patients was separated into ideal group (n = 31) and average group (n = 15).
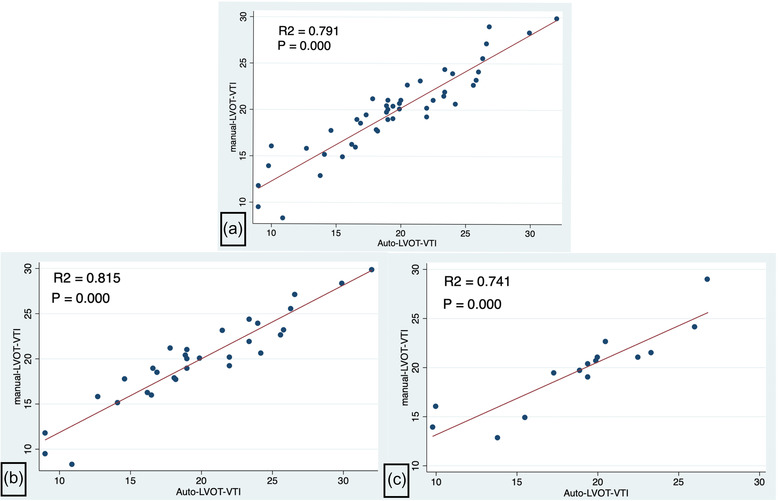
Left ventricular end-diastolic dimension (LVEDd, p = 0.1028), left ventricular ejection fraction (LVEF, p = 0.3251), left atrial dimension (LA-d, p = 0.0962), left ventricular E/A ratio (p = 0.160), left ventricular wall motion (p = 0.317) and pericardial effusion (p = 1) had no significant difference between trained ICU doctors and expert sonographer. ICU patients in average group had greater sequential organ failure assessment (SOFA) score (7.33 ± 1.58 vs. 4.09 ± 0.57, p = 0.022) and lactic acid (3.67 ± 0.86 mmol/L vs. 1.46 ± 0.12 mmol/L, p = 0.0009) with greater value of LVEDd (51.93 ± 1.07 vs. 47.57 ± 0.89, p = 0.0053), LA-d (39.06 ± 1.47 vs. 35.22 ± 0.98, p = 0.0334) and percentage of decreased wall motion (p = 0.0166) than ideal group. There were no significant differences of δLVOT-VTI (|manual LVOT-VTI - auto LVOT-VTI|/manual VTI*100%) between the two groups (8.8% ± 1.3% vs. 10% ± 2%, p = 0.6517). Statistically, significant correlations between manual LVOT-VTI and auto LVOT-VTI were present in the ideal group (R = 0.815, p = 0.00) and average group (R = 0.741, p = 0.00).
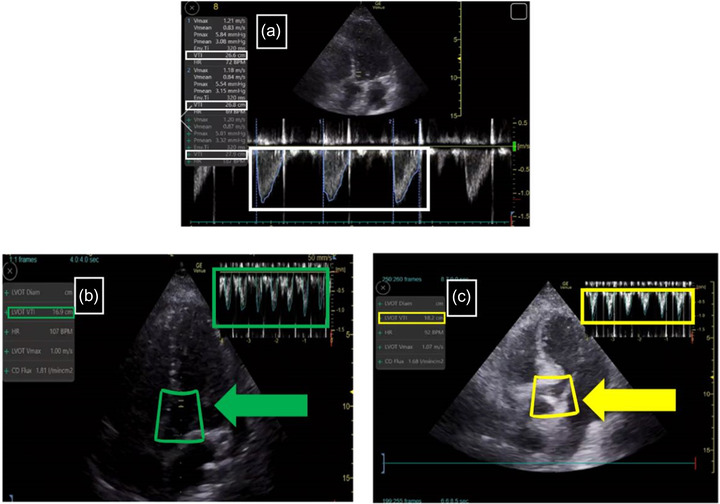
ICU doctors could achieve the satisfied level of expertise as expert sonographers after 3 months of PoCUS training. Nearly two thirds of the enrolled ICU doctors could obtain the ideal view and one third of them could acquire the average view. ICU patients with higher SOFA scores and lactic acid were less likely to acquire the ideal view. Manual and auto LVOT-VTI had statistically significant agreement in both ideal and average groups. Auto LVOT-VTI in ideal view was more relevant with the manual LVOT-VTI than the average view. AI might provide real-time guidance among novice operators who lack expertise to acquire the ideal standard view.
床边超声心动图(PoCUS)在医学教育中的应用是一个相对较新的课程。在床边超声教育的存在、数量、提供和深度方面仍存在很大差异。左心室流出道速度时间积分(LVOT-VTI)已成功用于几项研究中,作为评估危重病患者血流动力学管理的参数,尤其是在评估液体反应性方面。虽然 LVOT-VTI 已经得到广泛应用,但在 PoCUS 中使用人工智能(AI)的有价值的应用仍然有限。我们的目的是确定自动 LVOT-VTI 与经过 PoCUS 培训的 ICU 医生手动获取的 LVOT-VTI 之间的相关性程度。
在 2019 年 9 月 1 日至 2020 年 11 月 30 日期间参加 PoCUS 培训的 58 名 ICU 医生中,选择接受培训超过 3 个月的 46 名 ICU 医生作为研究对象。在 PoCUS 培训结束时,每位入组的 ICU 医生在新患者入院后 2 小时内获取新 ICU 患者的超声心动图参数。两名床边专家超声医师中的一位会在 24 小时内对新 ICU 患者进行标准超声心动图检查。对于 ICU 医生,参考手动 LVOT-VTI,并使用 AI 软件工具即时计算自动 LVOT-VTI。根据自动 LVOT-VTI 的图像质量,将 ICU 患者分为理想组(n=31)和平均组(n=15)。
左心室舒张末期内径(LVEDd,p=0.1028)、左心室射血分数(LVEF,p=0.3251)、左心房内径(LA-d,p=0.0962)、左心室 E/A 比值(p=0.160)、左心室壁运动(p=0.317)和心包积液(p=1)在经过培训的 ICU 医生和专家超声医师之间没有显著差异。平均组 ICU 患者的序贯器官衰竭评估(SOFA)评分更高(7.33±1.58 vs. 4.09±0.57,p=0.022),乳酸水平更高(3.67±0.86mmol/L vs. 1.46±0.12mmol/L,p=0.0009),LVEDd 值更大(51.93±1.07 vs. 47.57±0.89,p=0.0053),LA-d 值更大(39.06±1.47 vs. 35.22±0.98,p=0.0334),壁运动减少的百分比更大(p=0.0166),与理想组相比。两组间的δLVOT-VTI(|手动 LVOT-VTI - 自动 LVOT-VTI|/手动 VTI*100%)无显著差异(8.8%±1.3% vs. 10%±2%,p=0.6517)。在理想组(R=0.815,p=0.00)和平均组(R=0.741,p=0.00)中,手动 LVOT-VTI 和自动 LVOT-VTI 之间存在统计学显著相关性。
经过 3 个月的 PoCUS 培训,ICU 医生可以达到与专家超声医师相当的专业水平。入组的 ICU 医生中有近三分之二可以获得理想的视图,三分之一可以获得平均视图。SOFA 评分和乳酸水平较高的 ICU 患者不太可能获得理想的视图。理想组和平均组中手动和自动 LVOT-VTI 具有统计学显著的一致性。理想视图中的自动 LVOT-VTI 与手动 LVOT-VTI 的相关性大于平均视图。AI 可能为缺乏专业知识的新手操作员提供实时指导,以获取理想的标准视图。