Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, The University of Oxford, West Wing Level 6, Oxford, OX3 9DU, UK.
Oxford Spine Service, Nuffield Orthopaedic Centre, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
Eur Spine J. 2023 Feb;32(2):517-533. doi: 10.1007/s00586-022-07356-y. Epub 2022 Dec 29.
Physiotherapy interventions are prescribed as first-line treatment for people with sciatica; however, their effectiveness remains controversial. The purpose of this systematic review was to establish the short-, medium- and long-term effectiveness of physiotherapy interventions compared to control interventions for people with clinically diagnosed sciatica.
This systematic review was registered on PROSPERO CRD42018103900. Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL (EBSCO), Embase, PEDro, PubMed, Scopus and grey literature were searched from inception to January 2021 without language restrictions. Inclusion criteria were randomised controlled trials evaluating physiotherapy interventions compared to a control intervention in people with clinical or imaging diagnosis of sciatica. Primary outcome measures were pain and disability. Study selection and data extraction were performed by two independent reviewers with consensus reached by discussion or third-party arbitration if required. Risk of bias was assessed independently by two reviewers using the Cochrane Risk of Bias tool with third-party consensus if required. Meta-analyses and sensitivity analyses were performed with random effects models using Revman v5.4. Subgroup analyses were undertaken to examine the effectiveness of physiotherapy interventions compared to minimal (e.g. advice only) or substantial control interventions (e.g. surgery).
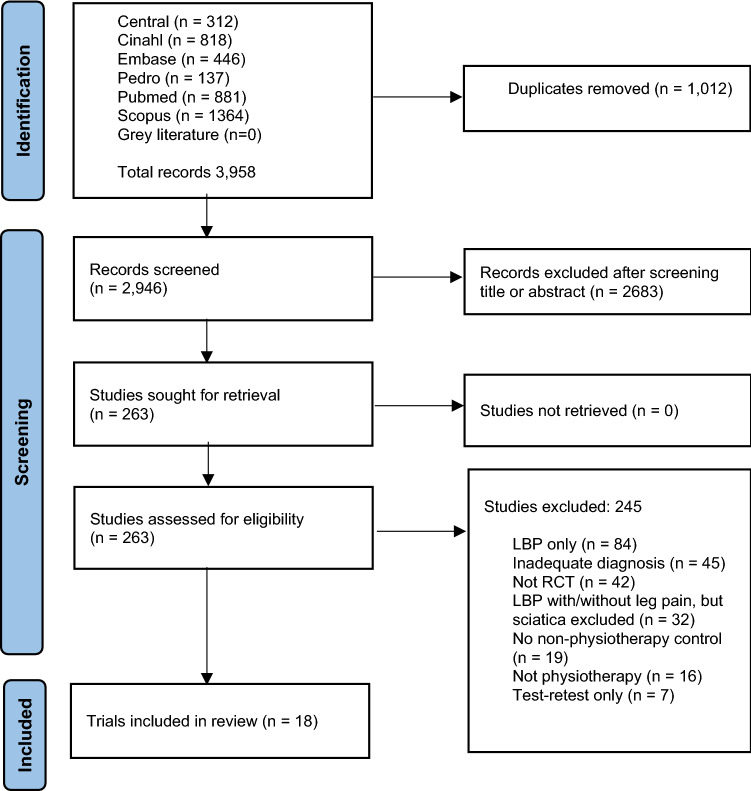
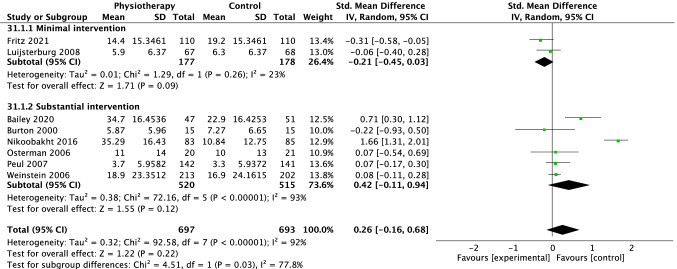
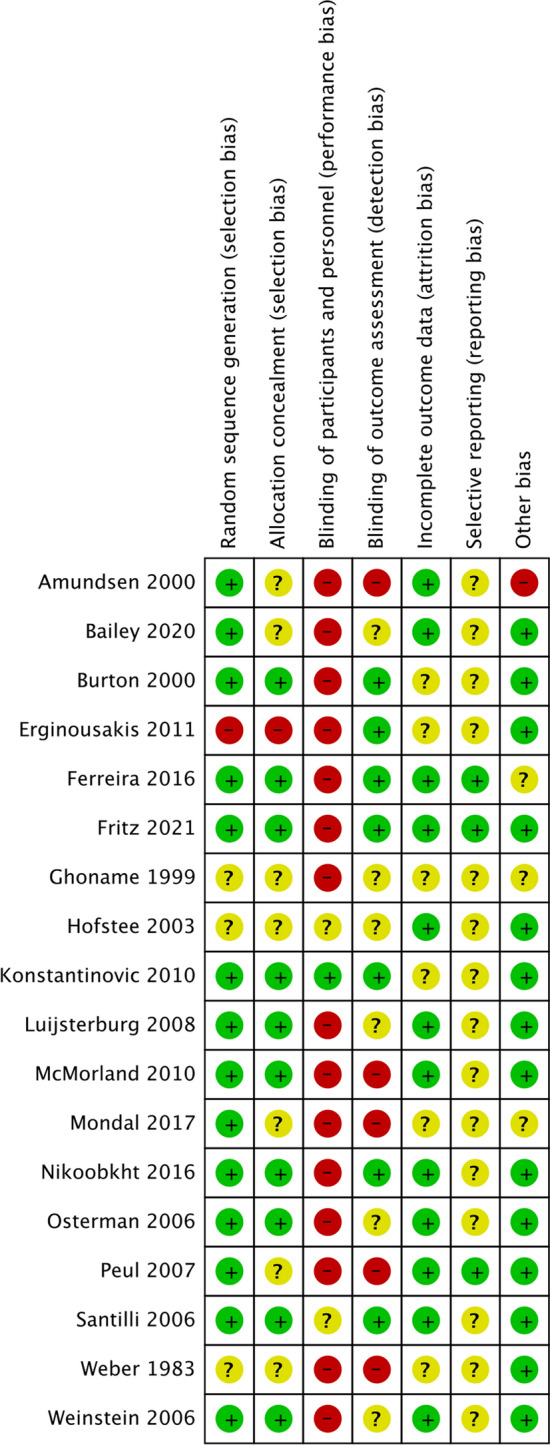
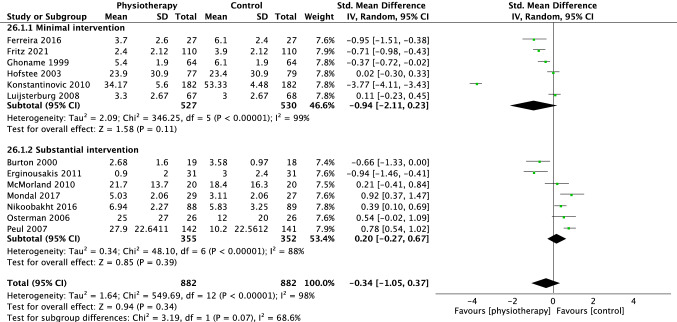
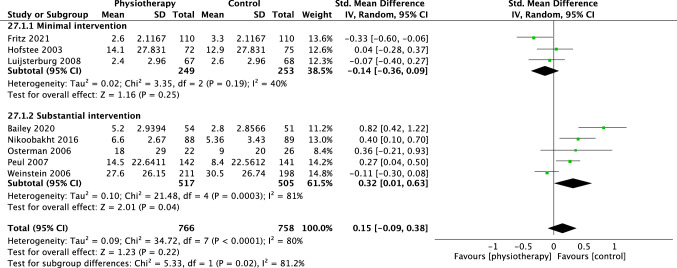
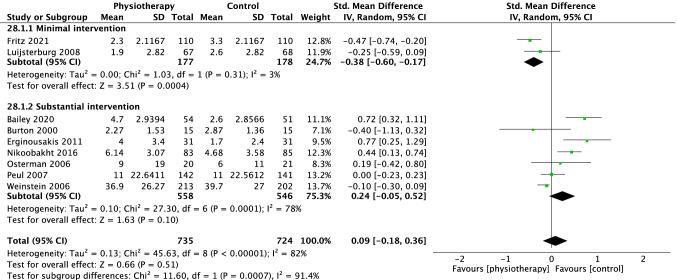
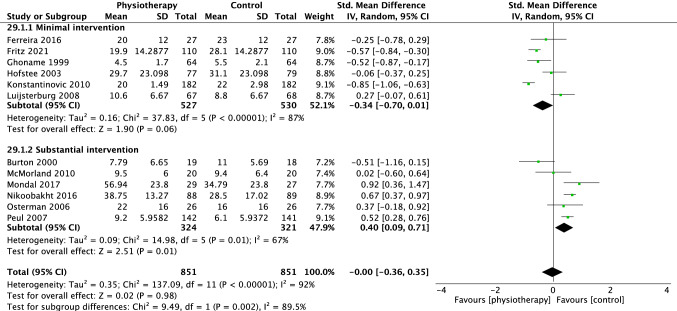
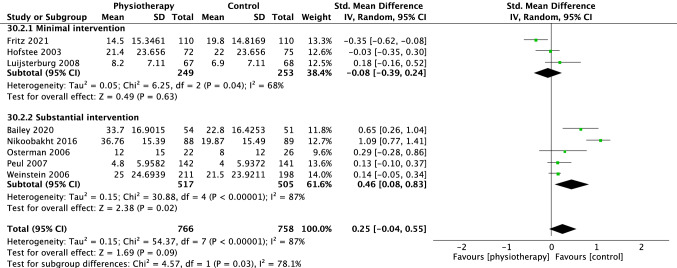
Three thousand nine hundred and fifty eight records were identified, of which 18 trials were included, with a total number of 2699 participants. All trials had a high or unclear risk of bias. Meta-analysis of trials for the outcome of pain showed no difference in the short (SMD - 0.34 [95%CI - 1.05, 0.37] p = 0.34, I = 98%), medium (SMD 0.15 [95%CI - 0.09, 0.38], p = 0.22, I= 80%) or long term (SMD 0.09 [95%CI - 0.18, 0.36], p = 0.51, I= 82%). For disability there was no difference in the short (SMD - 0.00 [95%CI - 0.36, 0.35], p = 0.98, I = 92%, medium (SMD 0.25 [95%CI - 0.04, 0.55] p = 0.09, I = 87%), or long term (SMD 0.26 [95%CI - 0.16, 0.68] p = 0.22, I = 92%) between physiotherapy and control interventions. Subgroup analysis of studies comparing physiotherapy with minimal intervention favoured physiotherapy for pain at the long-term time points. Large confidence intervals and high heterogeneity indicate substantial uncertainly surrounding these estimates. Many trials evaluating physiotherapy intervention compared to substantial intervention did not use contemporary physiotherapy interventions.
Based on currently available, mostly high risk of bias and highly heterogeneous data, there is inadequate evidence to make clinical recommendations on the effectiveness of physiotherapy interventions for people with clinically diagnosed sciatica. Future studies should aim to reduce clinical heterogeneity and to use contemporary physiotherapy interventions.
物理治疗干预被规定为坐骨神经痛患者的一线治疗方法;然而,其疗效仍存在争议。本系统评价的目的是确定与对照干预相比,物理治疗干预在临床诊断为坐骨神经痛的患者中的短期、中期和长期疗效。
本系统评价已在 PROSPERO CRD42018103900 上注册。对 Cochrane 对照试验中央注册库(CENTRAL)、CINAHL(EBSCO)、Embase、PEDro、PubMed、Scopus 和灰色文献进行了检索,检索时间从开始到 2021 年 1 月,无语言限制。纳入标准为评估物理治疗干预与临床或影像学诊断为坐骨神经痛的对照干预相比的随机对照试验。主要结局指标为疼痛和残疾。两名独立评审员进行了研究选择和数据提取,如果需要,可通过第三方仲裁达成共识。两名评审员使用 Cochrane 偏倚风险工具独立评估偏倚风险,如果需要,可通过第三方达成共识。使用 Revman v5.4 进行随机效应模型的荟萃分析和敏感性分析。进行亚组分析以检验物理治疗干预与最小(例如仅提供建议)或较大(例如手术)对照干预相比的疗效。
共确定了 3958 条记录,其中 18 项试验被纳入,共有 2699 名参与者。所有试验均具有高或不明确的偏倚风险。对疼痛结局的试验进行荟萃分析显示,短期(SMD-0.34 [95%CI-1.05, 0.37],p=0.34,I=98%)、中期(SMD 0.15 [95%CI-0.09, 0.38],p=0.22,I=80%)或长期(SMD 0.09 [95%CI-0.18, 0.36],p=0.51,I=82%)的差异无统计学意义。在残疾方面,短期(SMD-0.00 [95%CI-0.36, 0.35],p=0.98,I=92%)、中期(SMD 0.25 [95%CI-0.04, 0.55],p=0.09,I=87%)或长期(SMD 0.26 [95%CI-0.16, 0.68],p=0.22,I=92%)的差异均无统计学意义。与对照组相比,物理治疗与最小干预的亚组分析对疼痛的长期疗效更有利。较大的置信区间和高度的异质性表明,这些估计存在很大的不确定性。许多评估物理治疗干预与较大干预相比的试验并未使用现代物理治疗干预。
基于目前可用的、主要为高偏倚风险和高度异质性的数据,尚无充分证据可对临床诊断为坐骨神经痛患者的物理治疗干预的疗效做出临床推荐。未来的研究应旨在减少临床异质性并使用现代物理治疗干预。