Gastrointestinal and Liver Diseases Division, Keck Medicine of University of Southern California, Los Angeles, California, USA.
Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan, USA.
Am J Gastroenterol. 2023 Jul 1;118(7):1214-1225. doi: 10.14309/ajg.0000000000002125. Epub 2022 Dec 23.
Hepatitis B surface antigen (HBsAg) loss is associated with improved long-term outcomes of patients with chronic hepatitis B but is infrequently achieved with current monotherapies. We assessed whether combination strategies that included treatment withdrawal enhanced HBsAg loss.
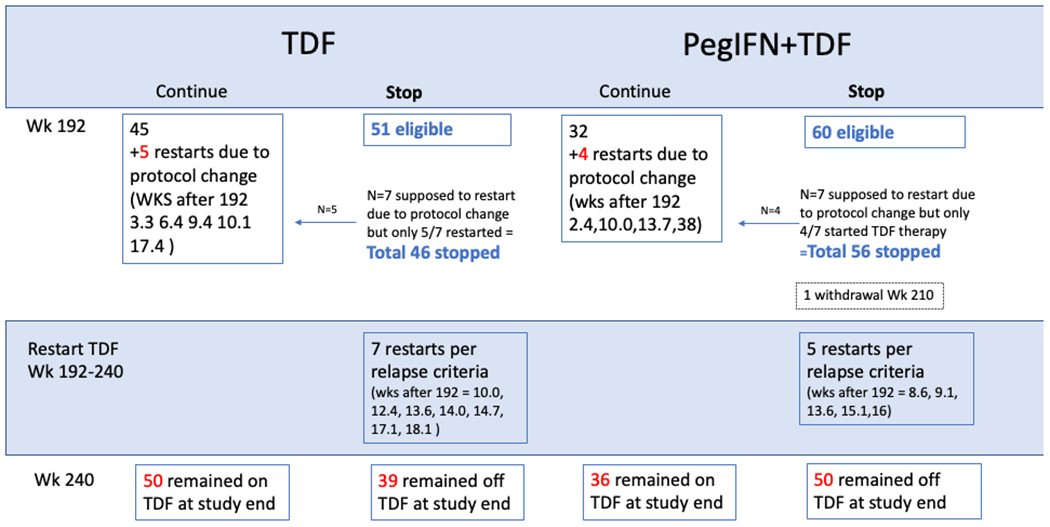
A randomized (1:1) trial of tenofovir disoproxil fumarate (TDF) for 192 weeks with or without peginterferon (PegIFN) alfa-2a for the first 24 weeks, followed by withdrawal of TDF at week 192 with 48 weeks of off-treatment follow-up to week 240. The primary end point was HBsAg loss at week 240.
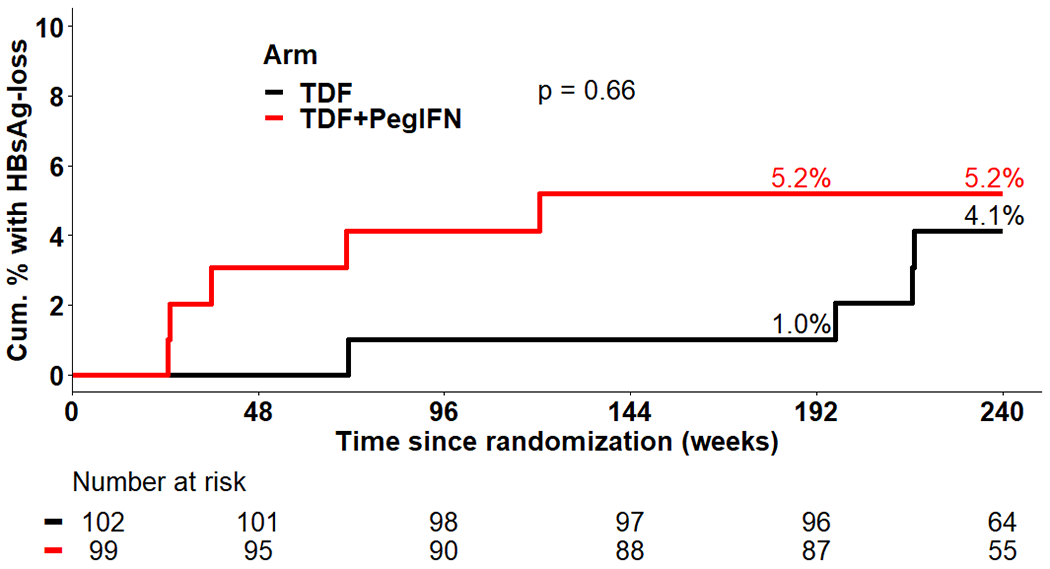
Of 201 participants (52% HBeAg positive, 12%/6% genotype A/A2, 7% cirrhosis) randomized to TDF + PegIFN (n = 102) or TDF alone (n = 99), 6 participants had lost HBsAg at the end of the treatment phase (week 192), 5 (5.3%) in the combination group, and 1 (1.0%) in the TDF alone group ( P = 0.09). By week 240, 9 participants had cleared HBsAg, 5.3% in combination, and 4.1% in monotherapy arms ( P = 0.73). HBsAg decline and loss occurred earlier with TDF + PegIFN than TDF, with a ≥1-logIU/mL qHBsAg decline by week 24 in 28% in TDF + PegIFN compared with 6% in TDF ( P = 0.04). HBsAg loss occurred in 7 of 12 (58%) with hepatitis B virus subgenotype A2 (all HBeAg positive) compared with only 2 of 189 (1%) with other hepatitis B virus genotypes and in 8 of 93 (8.6%) HBeAg positive vs 1 of 87 (1.1%) HBeAg negative.
PegIFN combined TDF followed by protocolized TDF withdrawal led to earlier but not higher percentages of HBsAg clearance. Pretreatment HBeAg positivity and subgenotype A2 were strongly associated with HBsAg clearance.
乙肝表面抗原(HBsAg)的丢失与慢性乙型肝炎患者的长期预后改善相关,但目前的单药治疗很少能实现这一目标。我们评估了包括停药在内的联合治疗策略是否能增强 HBsAg 的丢失。
使用替诺福韦酯(TDF)进行为期 192 周的随机(1:1)试验,前 24 周加用聚乙二醇干扰素(PegIFN)α-2a,第 192 周时停用 TDF,停药后进行 48 周的随访,直至第 240 周。主要终点是第 240 周时 HBsAg 的丢失。
在 201 名参与者(52%HBeAg 阳性,12%/6%基因型 A/A2,7%肝硬化)中,102 名随机接受 TDF+PegIFN 治疗,99 名接受 TDF 单药治疗。在治疗结束时(第 192 周),有 6 名参与者的 HBsAg 丢失,联合组 5 名(5.3%),TDF 单药组 1 名(1.0%)(P=0.09)。到第 240 周时,有 9 名参与者清除了 HBsAg,联合组 5.3%,单药组 4.1%(P=0.73)。与 TDF 相比,TDF+PegIFN 更早地出现 HBsAg 下降和丢失,联合组在第 24 周时 qHBsAg 下降≥1logIU/mL 的比例为 28%,而 TDF 组为 6%(P=0.04)。HBsAg 丢失发生在 12 名乙型肝炎病毒亚基因型 A2 的患者中的 7 名(58%),而其他乙型肝炎病毒基因型的患者中只有 189 名中的 2 名(1%),在 93 名 HBeAg 阳性的患者中发生了 8 例(8.6%),而在 87 名 HBeAg 阴性的患者中只有 1 例(1.1%)。
TDF 联合 PegIFN 后按方案停药导致 HBsAg 清除率更早但不更高。治疗前 HBeAg 阳性和亚基因型 A2 与 HBsAg 清除有很强的相关性。