Agency for Healthcare Research and Quality, Rockville, Maryland.
McCourt School of Public Health, Georgetown University, Washington, DC.
JAMA Netw Open. 2023 Jan 3;6(1):e2244975. doi: 10.1001/jamanetworkopen.2022.44975.
Multisystem inflammatory syndrome in children (MIS-C) causes severe inflammation of multiple organ systems after SARS-CoV-2 infection. During the pandemic, surveillance reporting of MIS-C was voluntary, with likely underreporting. For a rare syndrome like MIS-C, numerous data are needed to explore the disease in greater detail.
To use large all-payer billing data and the new International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Clinical Modification (ICD-10-CM) code for MIS-C to compare outcomes across MIS-C and COVID-19 over all 4057 hospitals in 31 states.
DESIGN, SETTING, AND PARTICIPANTS: A retrospective cross-sectional study of all COVID-19 and MIS-C hospitalizations in individuals younger than 21 years from 31 states was conducted, using Agency for Healthcare Research and Quality 2021 Healthcare Cost and Utilization Project data. Analyses were conducted from February 1 to October 20, 2022.
Fifty complications, adverse medication events, costs, and the Social Vulnerability Index.
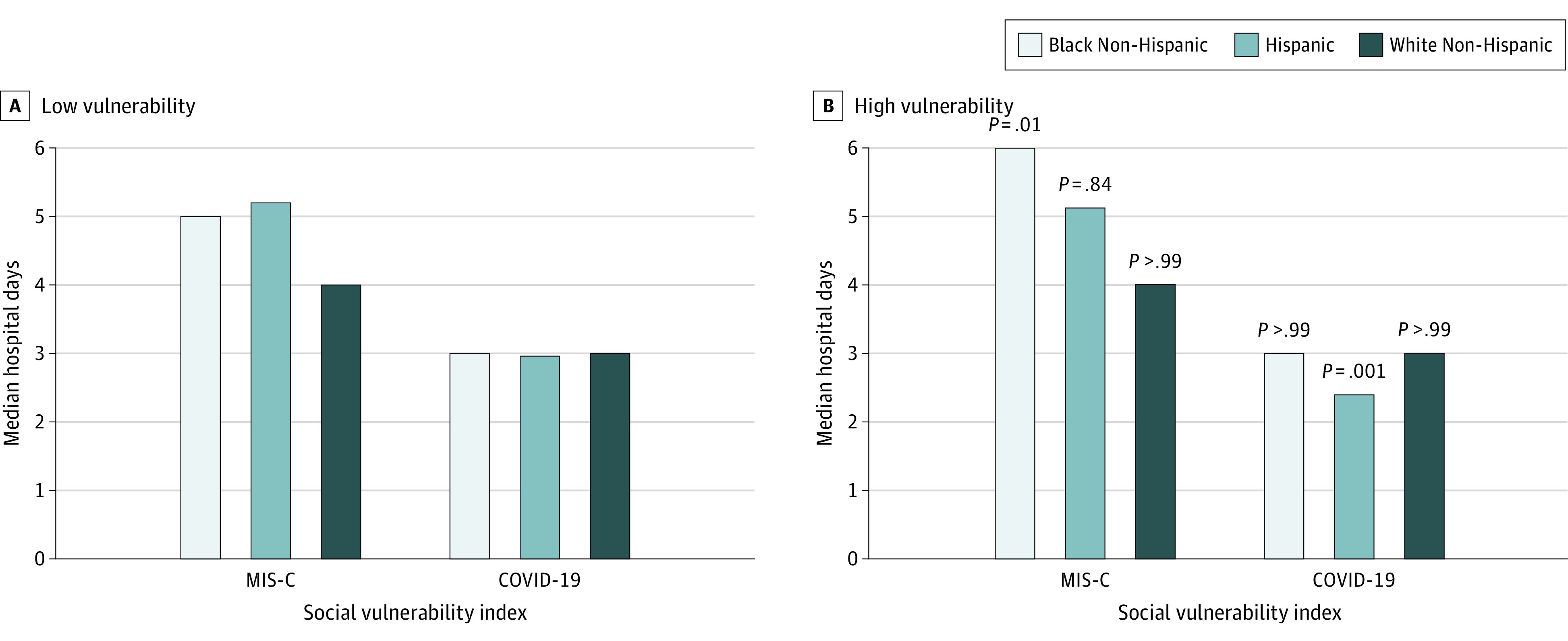
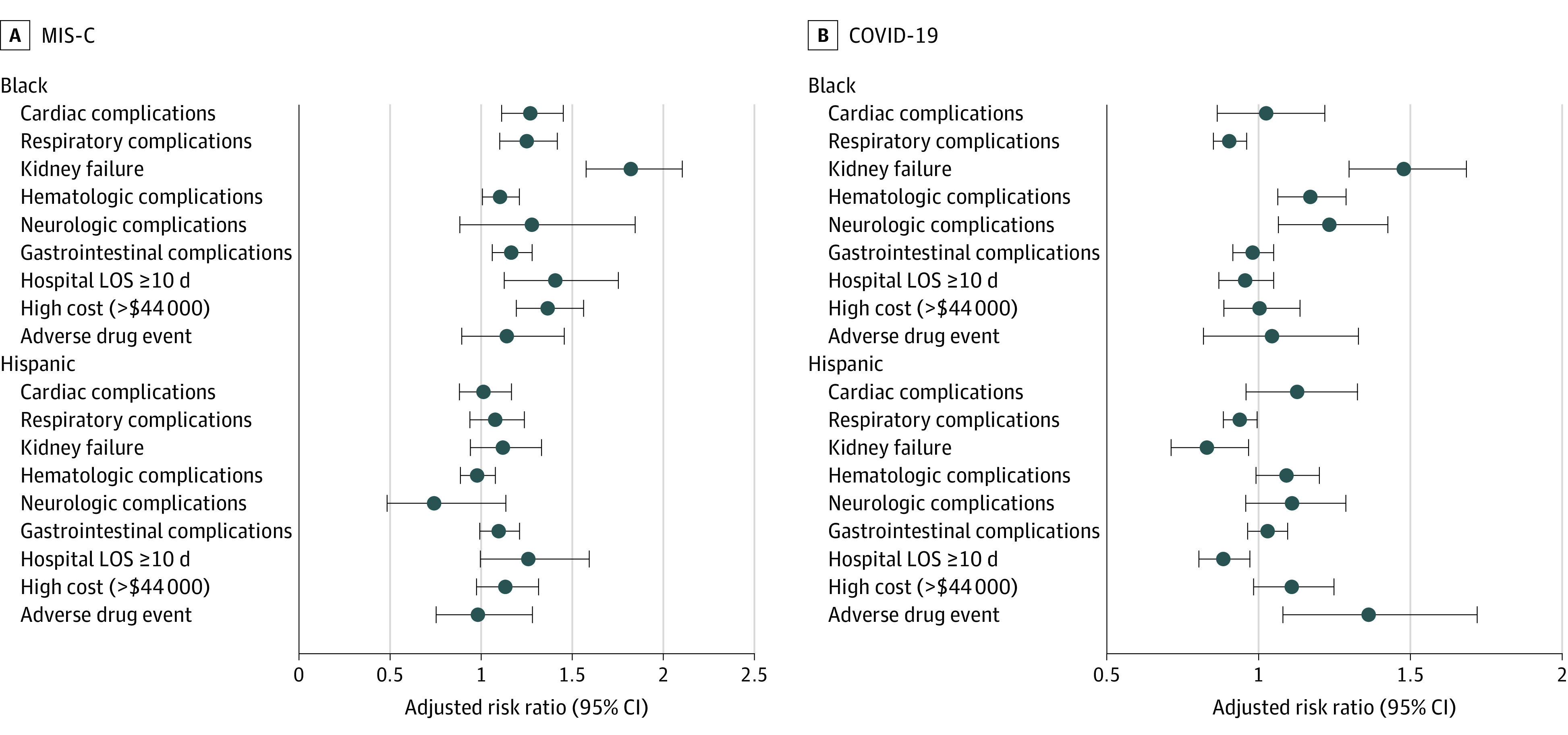
There were 4107 individuals with MIS-C (median age, 9 [IQR, 5-13] years; 2443 [59.5%] male; 1384 [38.1%] White) and 23 686 individuals with COVID-19 without MIS-C (median age, 15 [IQR, 5-18] years; 12 878 [54.4%] female; 4605 [44.1%] White), with 1.48 (95% CI, 1.35-1.62) MIS-C hospitalizations per 100 000 children per month, ranging from 0.97 hospitalizations per 100 children for White and 1.99 hospitalizations per 100 children for Black children. Outcomes worsened as the number of organ system dysfunctions increased from 2 to 8 organs. Deaths associated with MIS-C increased from less than 1% to 5.8% (95% CI, 3.3%-8.4%) and from less than 1% to 17.2% (95% CI, 11.7%-22.7%) for COVID-19 (P = .001). Adverse medication events associated with MIS-C increased from 4.9% (95% CI, 3.8%-6.0%) to 17.8% (95% CI, 13.7%-22.0%) and from 1.2% (95% CI, 1.0%-1.3%) to 13.4% (95% CI, 8.4%-18.3%) for COVID-19. The median length of stay for MIS-C increased from 4 (IQR, 2-5) to 8 (IQR, 5-12) days and from 3 (IQR, 2-5) to 16 (IQR, 7-23) days for COVID-19. Median costs for MIS-C increased from $16 225 (IQR, $9244-$26 822) to $53 359 (IQR, $35 920-$86 882) and from $6474 (IQR, $3741-$12 103) to $98 643 (IQR, $30 675-$204 956) for COVID-19. The percentage of MIS-C cases that were in Black children doubled from 16.2% to 31.7% (P = .001) as organ dysfunction increased, remaining unchanged with COVID-19. Hospital stays for MIS-C increased by 1 day (P = .01) for Black patients compared with White patients, with Black patients moving from the bottom to top quartile of socioeconomic vulnerability, with no disparity with COVID-19.
In this cross-sectional study, MIS-C was more common and severe than previously reported, with more racial disparities in outcomes than were seen in patients with COVID-19. The findings of this study suggest that relying on mean outcomes for MIS-C from past studies can be misleading, since outcomes and disparities varied widely with the number of multiorgan dysfunctions.
儿童多系统炎症综合征 (MIS-C) 是在 SARS-CoV-2 感染后多个器官系统严重炎症的表现。在大流行期间,MIS-C 的监测报告是自愿的,可能存在漏报。对于 MIS-C 这样的罕见综合征,需要大量数据来更详细地研究该疾病。
利用大型全付费账单数据和新的国际疾病分类和相关健康问题第十次修订版临床修正(ICD-10-CM)MIS-C 编码,在 31 个州的 4057 家医院中比较 MIS-C 和 COVID-19 之间的所有并发症、不良药物事件、成本和社会脆弱性指数。
设计、设置和参与者:这是一项回顾性的病例交叉研究,纳入了 31 个州年龄在 21 岁以下的所有 COVID-19 和 MIS-C 住院患者,使用了美国医疗保健研究与质量署 2021 年医疗保健成本和利用项目数据。分析于 2022 年 2 月 1 日至 10 月 20 日进行。
共纳入 4107 例 MIS-C(中位数年龄 9 [IQR,5-13]岁;2443 [59.5%]为男性;1384 [38.1%]为白人)和 23686 例无 MIS-C 的 COVID-19 患者(中位数年龄 15 [IQR,5-18]岁;12878 [54.4%]为女性;4605 [44.1%]为白人),每个月每 100000 名儿童有 1.48(95%CI,1.35-1.62)例 MIS-C 住院,范围从每 100 名儿童 0.97 例住院到每 100 名黑人儿童 1.99 例住院。随着器官功能障碍数量从 2 个增加到 8 个,结局恶化。与 MIS-C 相关的死亡从不到 1%增加到 5.8%(95%CI,3.3%-8.4%)和从不到 1%增加到 17.2%(95%CI,11.7%-22.7%),而与 COVID-19 相关的死亡从不到 1%增加到 17.2%(95%CI,11.7%-22.7%)(P=0.001)。与 MIS-C 相关的不良药物事件从 4.9%(95%CI,3.8%-6.0%)增加到 17.8%(95%CI,13.7%-22.0%),从 1.2%(95%CI,1.0%-1.3%)增加到 13.4%(95%CI,8.4%-18.3%),而与 COVID-19 相关的不良药物事件从 1.2%(95%CI,1.0%-1.3%)增加到 13.4%(95%CI,8.4%-18.3%)。MIS-C 的中位住院时间从 4(IQR,2-5)增加到 8(IQR,5-12)天,从 3(IQR,2-5)增加到 16(IQR,7-23)天,而 COVID-19 从 3(IQR,2-5)增加到 16(IQR,7-23)天。MIS-C 的中位费用从 16225 美元(IQR,9244-26822 美元)增加到 53359 美元(IQR,35920-86882 美元),从 6474 美元(IQR,3741-12103 美元)增加到 98643 美元(IQR,30675-204956 美元),而 COVID-19 的费用从 6474 美元(IQR,3741-12103 美元)增加到 98643 美元(IQR,30675-204956 美元)。随着器官功能障碍的增加,MIS-C 中黑人儿童的比例从 16.2%增加到 31.7%(P=0.001),而 COVID-19 中的黑人儿童比例保持不变。与白人患者相比,MIS-C 黑人患者的住院时间增加了 1 天(P=0.01),黑人患者从社会经济脆弱性的底层移到了顶层,与 COVID-19 没有差异。
在这项病例交叉研究中,MIS-C 比之前报道的更为常见和严重,与 COVID-19 相比,MIS-C 患者的结局存在更多的种族差异。本研究结果表明,依赖过去研究中 MIS-C 的平均结果可能会产生误导,因为结果和差异随多个器官功能障碍的数量而广泛变化。