Regional Intensive Care Unit, Royal Victoria Hospital, Belfast, UK.
Wellcome-Wolfson Institute for Experimental Medicine, Queen's University, Belfast, UK.
Crit Care. 2023 Jan 5;27(1):4. doi: 10.1186/s13054-022-04289-2.
Hypotension following out-of-hospital cardiac arrest (OHCA) may cause secondary brain injury and increase mortality rates. Current guidelines recommend avoiding hypotension. However, the optimal blood pressure following OHCA is unknown. We hypothesised that exposure to hypotension and hypertension in the first 24 h in ICU would be associated with mortality following OHCA.
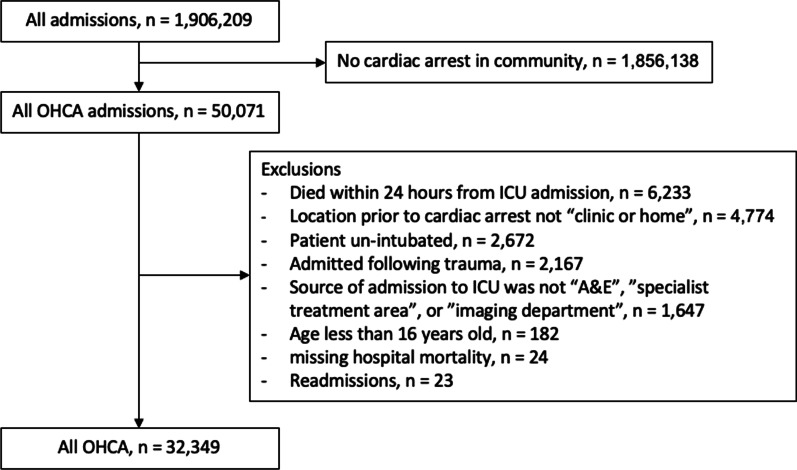
We conducted a retrospective analysis of OHCA patients included in the Intensive Care National Audit and Research Centre Case Mix Programme from 1 January 2010 to 31 December 2019. Restricted cubic splines were created following adjustment for important prognostic variables. We report the adjusted odds ratio for associations between lowest and highest mean arterial pressure (MAP) and systolic blood pressure (SBP) in the first 24 h of ICU care and hospital mortality.
A total of 32,349 patients were included in the analysis. Hospital mortality was 56.2%. The median lowest and highest MAP and SBP were similar in survivors and non-survivors. Both hypotension and hypertension were associated with increased mortality. Patients who had a lowest recorded MAP in the range 60-63 mmHg had the lowest associated mortality. Patients who had a highest recorded MAP in the range 95-104 mmHg had the lowest associated mortality. The association between SBP and mortality followed a similar pattern to MAP.
We found an association between hypotension and hypertension in the first 24 h in ICU and mortality following OHCA. The inability to distinguish between the median blood pressure of survivors and non-survivors indicates the need for research into individualised blood pressure targets for survivors following OHCA.
院外心脏骤停(OHCA)后低血压可能导致继发性脑损伤并增加死亡率。目前的指南建议避免低血压。然而,OHCA 后最佳血压尚不清楚。我们假设 ICU 内 24 小时内出现低血压和高血压与 OHCA 后的死亡率相关。
我们对 2010 年 1 月 1 日至 2019 年 12 月 31 日期间纳入重症监护国家审计和研究中心病例组合计划的 OHCA 患者进行了回顾性分析。在调整了重要预后变量后,创建了受限立方样条。我们报告了 ICU 护理前 24 小时内最低和最高平均动脉压(MAP)和收缩压(SBP)与医院死亡率之间关联的调整后比值比。
共纳入 32349 例患者。医院死亡率为 56.2%。幸存者和非幸存者的最低和最高 MAP 和 SBP 中位数相似。低血压和高血压均与死亡率增加相关。记录的最低 MAP 范围在 60-63mmHg 的患者死亡率最低。记录的最高 MAP 范围在 95-104mmHg 的患者死亡率最低。SBP 与死亡率之间的关联与 MAP 相似。
我们发现 ICU 内前 24 小时的低血压和高血压与 OHCA 后死亡率之间存在关联。幸存者和非幸存者的中位血压无法区分,表明需要研究 OHCA 后幸存者的个体化血压目标。