Department of Neurology, Taipei Veterans General Hospital, Taipei, Taiwan.
Department of Neurology, National Yang Ming Chiao Tung University School of Medicine, Taipei, Taiwan.
Ann Clin Transl Neurol. 2023 Mar;10(3):353-362. doi: 10.1002/acn3.51724. Epub 2023 Jan 6.
NIPA1 mutations have been implicated in hereditary spastic paraplegia (HSP) as the cause of spastic paraplegia type 6 (SPG6). The aim of this study was to investigate the clinical and genetic features of SPG6 in a Taiwanese HSP cohort.
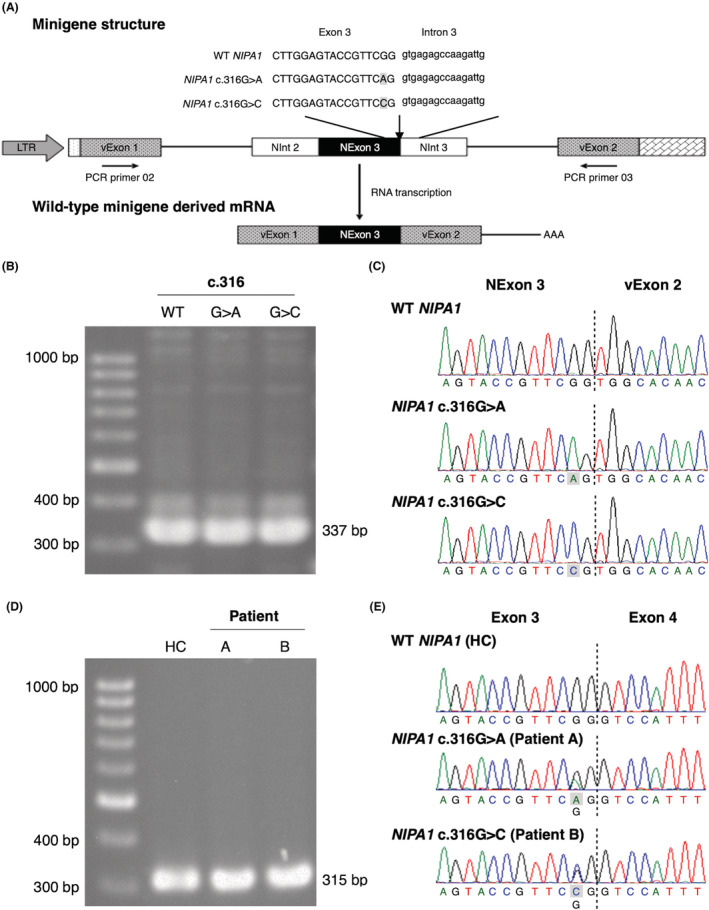
We screened 242 unrelated Taiwanese patients with HSP for NIPA1 mutations. The clinical features of patients with a NIPA1 mutation were analyzed. Minigene-based splicing assay, RT-PCR analysis on the patients' RNA, and cell-based protein expression study were utilized to assess the effects of the mutations on splicing and protein expression.
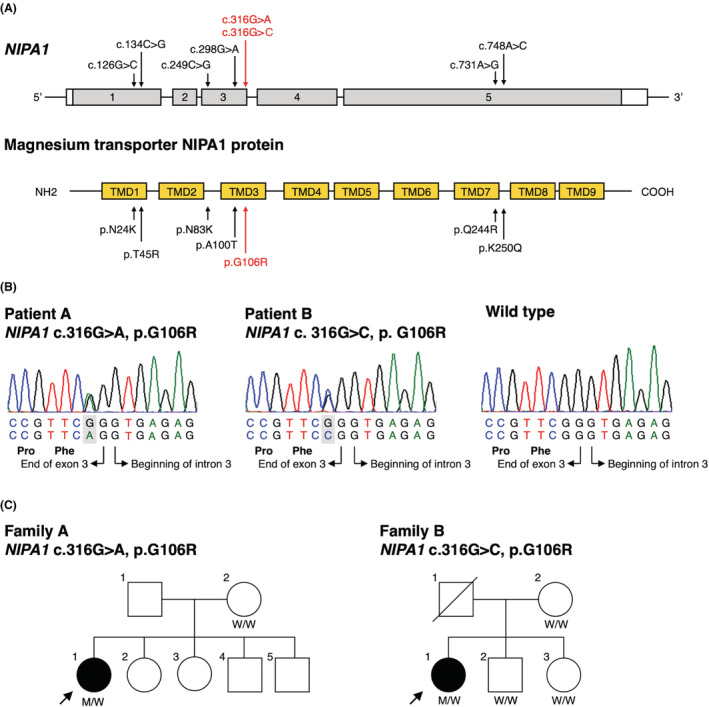
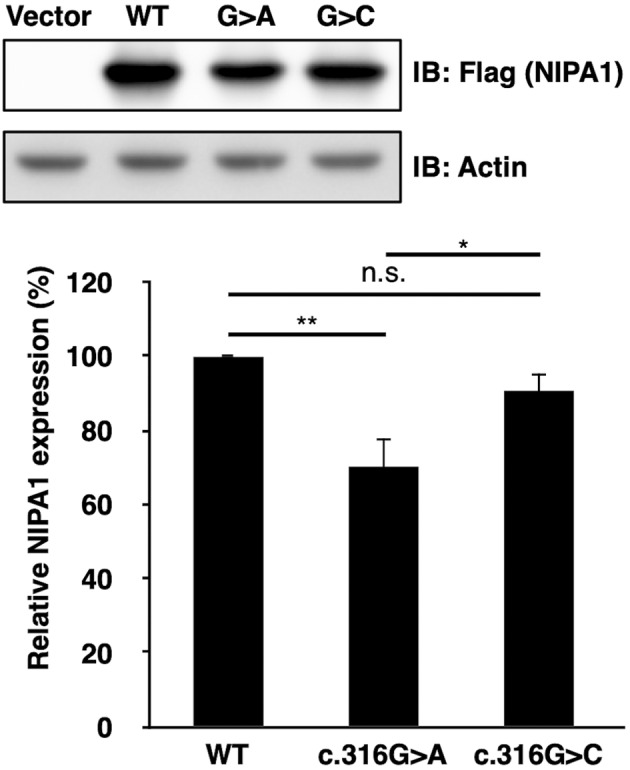
Two patients were identified to carry a different heterozygous NIPA1 mutation. The two mutations, c.316G>A and c.316G>C, are located in the 3' end of NIPA1 exon 3 near the exon-intron boundary and putatively lead to the same amino acid substitution, p.G106R. The patient harboring NIPA1 c.316G>A manifested spastic paraplegia, epilepsy and schizophrenia since age 17 years, whereas the individual carrying NIPA1 c.316G>C had pure HSP since age 12 years. We reviewed literature and found that epilepsy was present in multiple individuals with NIPA1 c.316G>A but none with NIPA1 c.316G>C. Functional studies demonstrated that both mutations did not affect splicing, but only the c.316G>A mutation was associated with a significantly reduced NIPA1 protein expression.
SPG6 accounted for 0.8% of HSP cases in the Taiwanese cohort. The NIPA1 c.316G>A and c.316G>C mutations are associated with adolescent-onset complex and pure form HSP, respectively. The different effects on protein expression of the two mutations may be associated with their phenotypic discrepancy.
NIPA1 突变已被认为是遗传性痉挛性截瘫(HSP)的致病原因,导致痉挛性截瘫 6 型(SPG6)。本研究旨在调查台湾 HSP 患者队列中 SPG6 的临床和遗传特征。
我们对 242 名无血缘关系的台湾 HSP 患者进行了 NIPA1 突变筛查。分析了携带 NIPA1 突变的患者的临床特征。利用基于微基因的剪接分析、患者 RNA 的 RT-PCR 分析以及基于细胞的蛋白表达研究,评估突变对剪接和蛋白表达的影响。
发现两名患者携带不同的杂合 NIPA1 突变。这两种突变,c.316G>A 和 c.316G>C,位于 NIPA1 外显子 3 的 3'端,靠近外显子-内含子边界,推测导致相同的氨基酸取代,p.G106R。携带 NIPA1 c.316G>A 的患者在 17 岁时出现痉挛性截瘫、癫痫和精神分裂症,而携带 NIPA1 c.316G>C 的患者在 12 岁时仅出现单纯 HSP。我们回顾了文献,发现 NIPA1 c.316G>A 中有多个个体出现癫痫,但 NIPA1 c.316G>C 中没有。功能研究表明,这两种突变都不影响剪接,但只有 c.316G>A 突变与 NIPA1 蛋白表达显著降低有关。
SPG6 在台湾 HSP 患者队列中占 0.8%。NIPA1 c.316G>A 和 c.316G>C 突变分别与青少年起病的复杂型和单纯型 HSP 有关。两种突变对蛋白表达的不同影响可能与其表型差异有关。