Department of General Surgery, Shengjing Hospital of China Medical University, Shenyang, China,
Department of General Surgery, Shengjing Hospital of China Medical University, Shenyang, China.
Digestion. 2023;104(2):85-96. doi: 10.1159/000528020. Epub 2023 Jan 6.
At present, endoscopic retrograde cholangiopancreatography (ERCP) and percutaneous transhepatic cholangial drainage (PTCD) are frequently used for reducing malignant obstructive jaundice (MOJ). However, it is controversial as to which method is superior in terms of efficacy and safety.
The aim of this study was to compare the safety, feasibility, and clinical benefits of ERCP and PTCD in matched cases of MOJ.
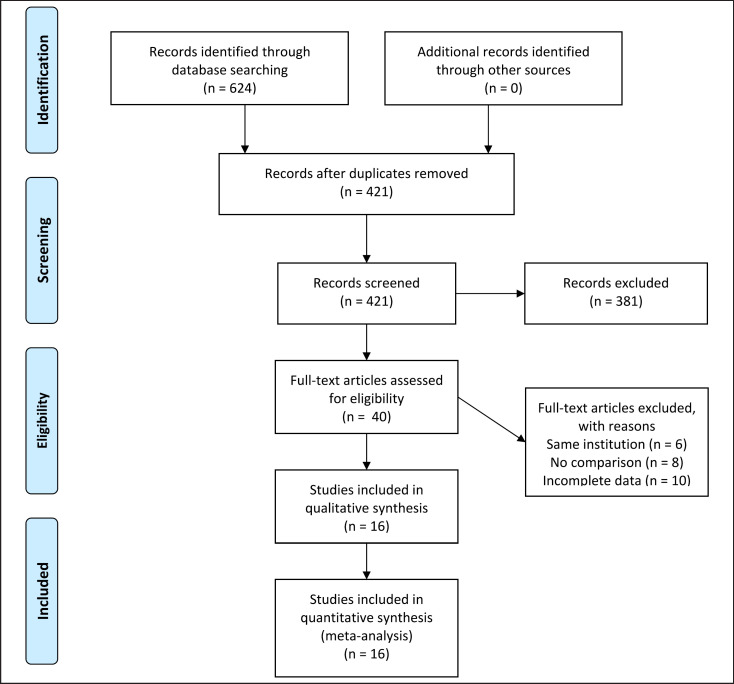
The Web of Science, Cochrane, PubMed, and CNKI databases were searched systematically to identify studies published between January 2000 and December 2019, without language restrictions, that compared ERCP and PTCD in patients with MOJ. The primary outcome was the success rate for each procedure. The secondary outcomes were the technical success rate, serum total bilirubin level, length of hospital stay, hospital expense, complication rate, and survival. This meta-analysis was performed using Review Manager 5.3.
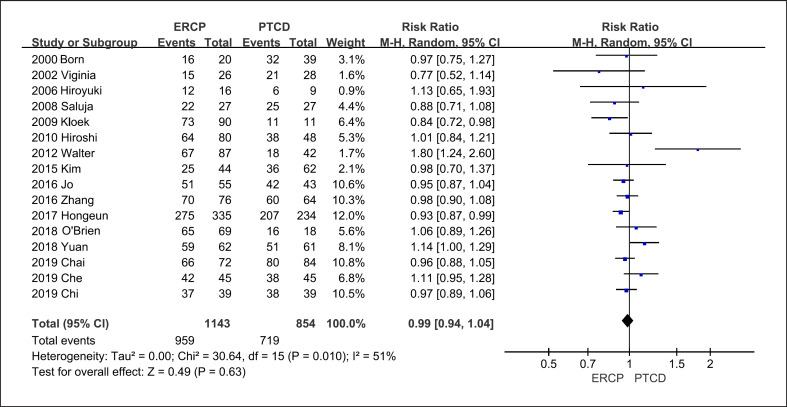
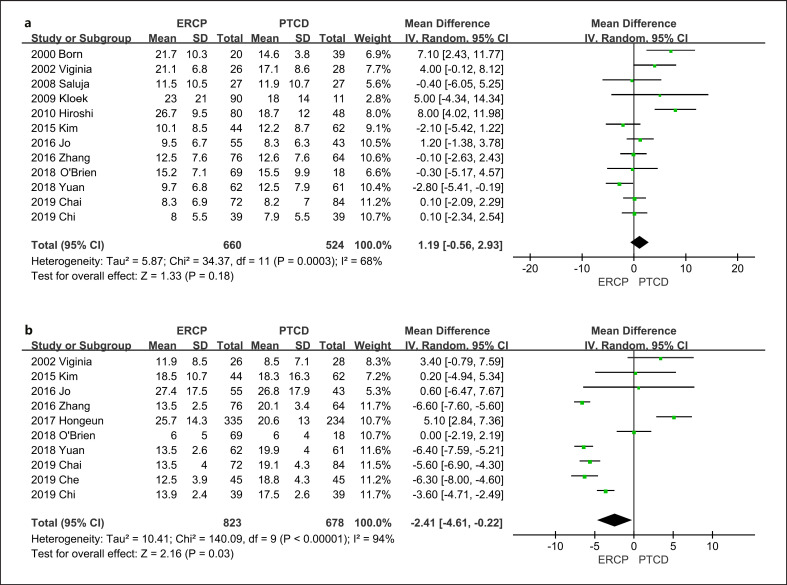
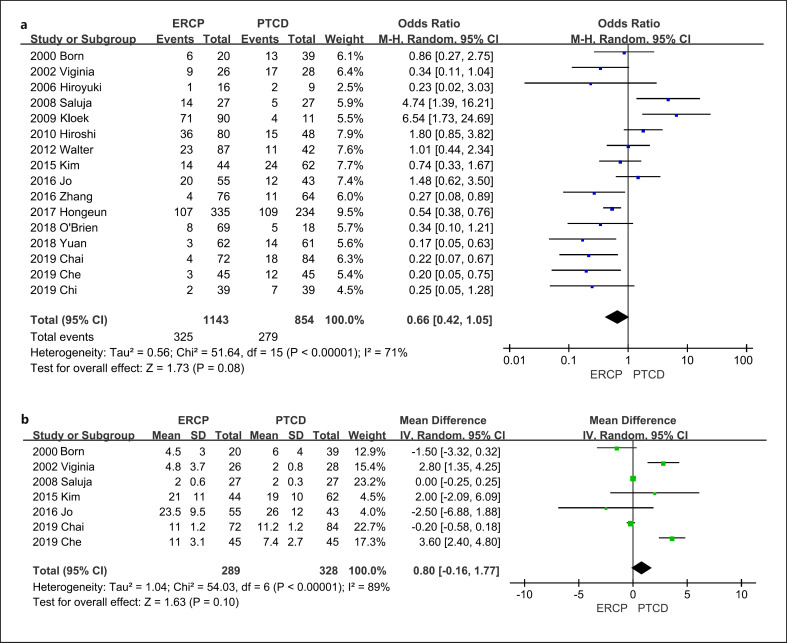
Sixteen studies met the inclusion criteria, including 1,143 cases of ERCP and 854 cases of PTCD. The analysis demonstrated that jaundice remission in PTCD was equal to that in ERCP (mean difference [MD], 1.19; 95% confidence interval [CI]: -0.56 to -2.93; p = 0.18). However, the length of hospital stay in the ERCP group was 3.03 days shorter than that in the PTCD group (MD, -2.41; 95% CI: -4.61 to -0.22; p = 0.03). ERCP had a lower rate of postoperative complications (odds ratio, 0.66; 95% CI: 0.42-1.05); however, the difference was not significant (p = 0.08). ERCP was also more cost-efficient (MD, -5.42; 95% CI: -5.52 to -5.32; p < 0.01). Further, we calculated the absolute mean of hospital stay (ERCP:PTCD = 8.73:12.95 days), hospital expenses (ERCP:PTCD = 5,104.13:5,866.75 RMB), and postoperative complications (ERCP:PTCD = 11.2%:9.1%) in both groups.
For remission of MOJ, PTCD and ERCP had similar clinical efficacy. Each method has its own strengths and weaknesses. Considering that ERCP had a lower rate of postoperative complications, shorter hospital stay, and higher cost efficiency, ERCP may be a superior initial treatment choice for MOJ.
目前,内镜逆行胰胆管造影术(ERCP)和经皮经肝胆管引流术(PTCD)常用于降低恶性梗阻性黄疸(MOJ)。然而,哪种方法在疗效和安全性方面更具优势仍存在争议。
本研究旨在比较 MOJ 匹配病例中 ERCP 和 PTCD 的安全性、可行性和临床获益。
系统检索 2000 年 1 月至 2019 年 12 月期间发表的英文和中文文献,纳入比较 MOJ 患者 ERCP 和 PTCD 的研究,不限制语言。主要结局指标为每种操作的成功率。次要结局指标为技术成功率、血清总胆红素水平、住院时间、住院费用、并发症发生率和生存率。采用 Review Manager 5.3 进行荟萃分析。
纳入 16 项研究,共 1143 例 ERCP 组和 854 例 PTCD 组。分析结果显示,PTCD 组黄疸缓解率与 ERCP 组相当(平均差值 [MD],1.19;95%置信区间 [CI]:-0.56 至 -2.93;p = 0.18)。然而,ERCP 组的住院时间比 PTCD 组短 3.03 天(MD,-2.41;95% CI:-4.61 至 -0.22;p = 0.03)。ERCP 的术后并发症发生率较低(比值比,0.66;95% CI:0.42-1.05);但差异无统计学意义(p = 0.08)。ERCP 也更具成本效益(MD,-5.42;95% CI:-5.52 至 -5.32;p < 0.01)。此外,我们计算了两组的住院时间绝对平均值(ERCP:PTCD = 8.73:12.95 天)、住院费用(ERCP:PTCD = 5104.13:5866.75 人民币)和术后并发症发生率(ERCP:PTCD = 11.2%:9.1%)。
对于 MOJ 的缓解,PTCD 和 ERCP 具有相似的临床疗效。每种方法都有其自身的优势和劣势。考虑到 ERCP 的术后并发症发生率较低、住院时间较短且成本效益较高,ERCP 可能是 MOJ 的首选初始治疗方法。