Van Der Westhuyzen M, Samodien N, Brink A J, Moodley C
Division of Medical Microbiology, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa.
National Health Laboratory Service, Microbiology, Groote Schuur Hospital, Cape Town, South Africa.
JAC Antimicrob Resist. 2023 Jan 4;5(1):dlac139. doi: 10.1093/jacamr/dlac139. eCollection 2023 Feb.
Determining lower respiratory tract infection (LRTI) aetiology is complex. Culture-based methods are laborious with poor sensitivity. Molecular assays improve detection of potential pathogens, but incorrect interpretation of results may lead to inappropriate antimicrobial therapy.
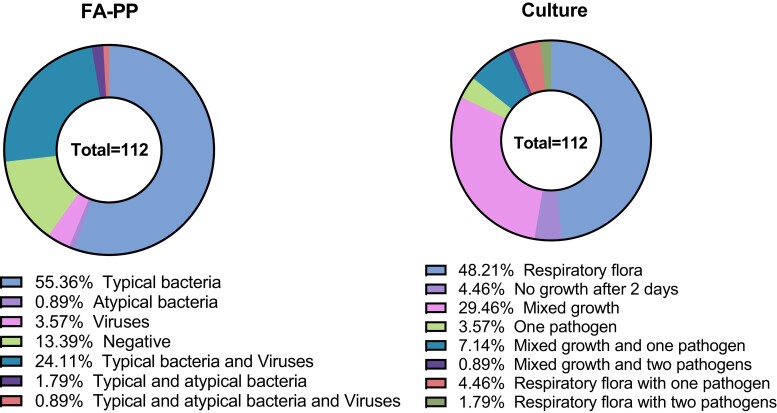
The utility of the BioFire FilmArray Pneumonia Panel (FA-PP) to detect LRTI pathogens, and the potential impact on antimicrobial stewardship in a low-resource setting, were assessed. Routine LRT samples were included from adult patients with clinically suspected LRTI or with a concomitant blood culture at Groote Schuur Hospital and referring facilities. Culture and FA-PP results were compared, and pharmacy data analysed to determine appropriateness of antibiotic therapy.
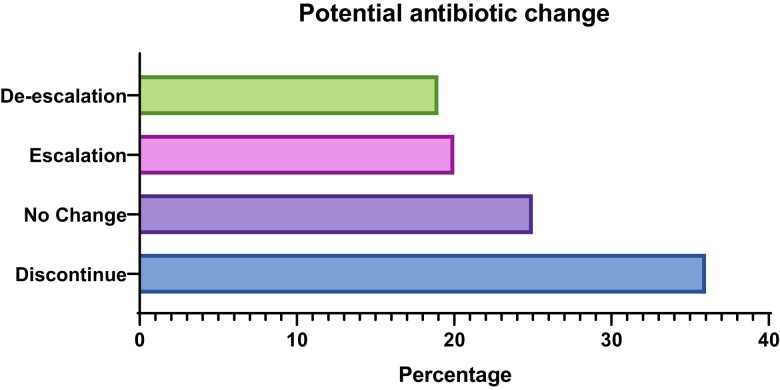
There was an 80% correlation between cultured LRTI pathogens and the FA-PP bin ≥10 results. Compared with culture, the FA-PP detected substantially more pathogens (86.6% versus 17.9%) and produced a combined 100% positive percent agreement, and 88% negative percent agreement. The FA-PP detected bacterial/viral coinfections in 27% of samples. Correlation of FA-PP results with pharmacy data ( = 69) indicated a potential antibiotic change in 75% of cases, but this is difficult to accurately characterize without a 'gold standard' for treatment or complete clinical data.
The FA-PP increased the number of positive samples with typical bacteria, but the semi-quantitative reporting algorithm does not describe the correlation between the different bin values and colonization versus infection. This complicates result interpretation and may lead to inappropriate antimicrobial treatment. This study highlights the potential positive impact of rapid molecular assays for routine care in lower-income settings, but also underscores the interpretive challenges associated with these tests.
确定下呼吸道感染(LRTI)的病因很复杂。基于培养的方法费力且灵敏度低。分子检测可提高潜在病原体的检测率,但结果解读错误可能导致不适当的抗菌治疗。
评估了BioFire FilmArray肺炎检测板(FA-PP)检测LRTI病原体的效用以及在资源匮乏环境中对抗菌药物管理的潜在影响。纳入了来自格罗特·舒尔医院及转诊机构的临床怀疑患有LRTI或同时进行血培养的成年患者的常规LRT样本。比较培养结果和FA-PP结果,并分析药房数据以确定抗生素治疗的适当性。
培养出的LRTI病原体与FA-PP分类≥10的结果之间存在80%的相关性。与培养相比,FA-PP检测到的病原体多得多(86.6%对17.9%),联合阳性百分比一致性为100%,阴性百分比一致性为88%。FA-PP在27%的样本中检测到细菌/病毒混合感染。FA-PP结果与药房数据(n = 69)的相关性表明,75%的病例可能需要更换抗生素,但在没有治疗“金标准”或完整临床数据的情况下,很难准确描述这一点。
FA-PP增加了典型细菌阳性样本的数量,但半定量报告算法未描述不同分类值与定植和感染之间的相关性。这使结果解读变得复杂,并可能导致不适当的抗菌治疗。本研究强调了快速分子检测对低收入环境中常规护理的潜在积极影响,但也强调了与这些检测相关的解读挑战。