Aung Kyaw L, McWhirter Elaine, Welch Stephen, Wang Lisa, Lovell Sophia, Stayner Lee-Anne, Ali Saara, Malpage Anne, Makepeace Barbara, Ramachandran Makilpriya, Jang Gun Ho, Gallinger Steven, Zhang Tong, Stockley Tracy L, Fischer Sandra E, Dhani Neesha, Hedley David, Knox Jennifer J, Siu Lillian L, Goodwin Rachel, Bedard Philippe L
Princess Margaret Cancer Centre, University Health Network, Toronto, ON, Canada.
Division of Medical Oncology & Hematology, Princess Margaret Cancer Centre, University Health Network, Department of Medicine, University of Toronto, Toronto, ON, Canada.
J Gastrointest Oncol. 2022 Dec;13(6):3216-3226. doi: 10.21037/jgo-22-86.
Mitogen-activated protein kinase kinase (MEK) is activated by mutated KRAS in >90% of pancreatic ductal adenocarcinoma (PDAC). MEK and focal adhesion kinase (FAK) are frequently co-activated in PDAC providing a rationale for combining trametinib, an oral allosteric MEK1/2 inhibitor, with GSK2256098, an oral FAK inhibitor.
Advanced PDAC patients whose disease progressed after first line palliative chemotherapy were treated with GSK2256098 250 mg twice daily and trametinib 0.5 mg once daily orally. The primary endpoint was clinical benefit (CB; complete response, partial response, or stable disease ≥24 weeks). Twenty-four patients were planned to enroll using a 2-stage minimax design (P=0.15, P=0.40; alpha =0.05, power 0.86). The combination would be considered inactive if 2/12 or fewer patients achieved CB at the end of stage 1, and would be considered active if >7/24 response-evaluable patients achieved CB by the end of stage 2. Serial blood samples were collected for circulating tumor DNA (ctDNA) mutation profiling.
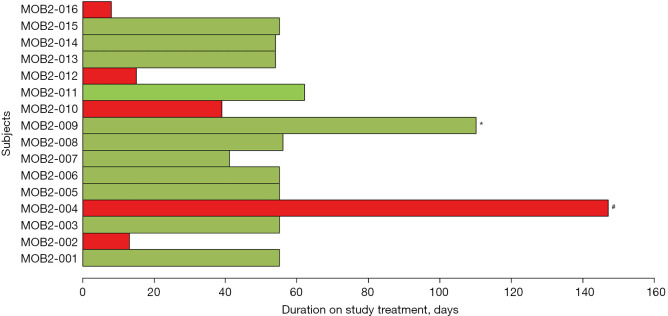
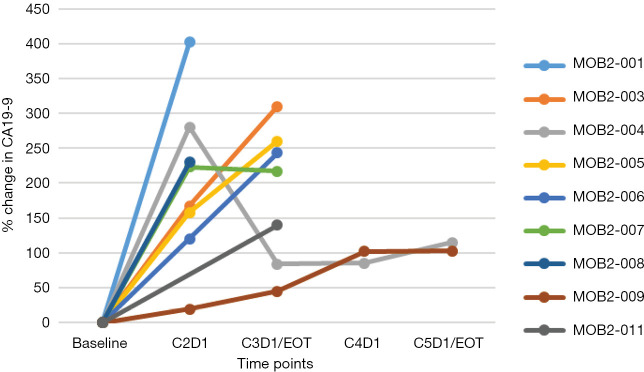
Sixteen patients were enrolled and 11 were response evaluable. Of those 11, 10 had progressive disease as best tumor response and one had stable disease for 4 months. No treatment related grade ≥3 adverse events (AEs) were observed. The median progression free survival (PFS) was 1.6 (95% CI: 1.5-1.8) months and the median overall survival (OS) was 3.6 (95% CI: 2.7-not reached) months. One response-inevaluable patient achieved clinical stability for 5 months with reduction in CA19-9 and ctDNA levels with a MAP2K1 treatment resistance mutation detected in ctDNA at clinical progression.
The combination of GSK2256098 and trametinib was well tolerated but was not active in unselected advanced PDAC.
在超过90%的胰腺导管腺癌(PDAC)中,丝裂原活化蛋白激酶激酶(MEK)由突变的KRAS激活。MEK和黏着斑激酶(FAK)在PDAC中经常共同激活,这为将口服变构MEK1/2抑制剂曲美替尼与口服FAK抑制剂GSK2256098联合使用提供了理论依据。
一线姑息化疗后疾病进展的晚期PDAC患者接受GSK2256098每日两次,每次250mg口服,曲美替尼每日一次,每次0.5mg口服治疗。主要终点是临床获益(CB;完全缓解、部分缓解或疾病稳定≥24周)。计划采用两阶段最小最大设计纳入24例患者(P = 0.15,P = 0.40;α = 0.05,检验效能0.86)。如果在第1阶段结束时2/12或更少患者达到CB,则认为该联合方案无效;如果在第2阶段结束时>7/24可评估反应的患者达到CB,则认为该联合方案有效。采集系列血样用于循环肿瘤DNA(ctDNA)突变分析。
纳入16例患者,其中11例可评估反应。在这11例患者中,10例最佳肿瘤反应为疾病进展,1例疾病稳定4个月。未观察到与治疗相关的≥3级不良事件(AE)。中位无进展生存期(PFS)为1.6(95%CI:1.5 - 1.8)个月,中位总生存期(OS)为3.6(95%CI:2.7 - 未达到)个月。1例不可评估反应的患者临床稳定5个月,CA19 - 9和ctDNA水平降低,临床进展时在ctDNA中检测到MAP2K1治疗耐药突变。
GSK2256098与曲美替尼联合耐受性良好,但在未选择的晚期PDAC中无活性。