Isaacson Sinéad, Kuczynski Kristine, Ormsby Nuchanart, Peay Holly L, Rennie Stuart, Cadigan R Jean, Kroon Eugène, Phanuphak Nittaya, Ananworanich Jintanat, Jupimai Thidarat, Prueksakaew Peeriya, Henderson Gail E
Social Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Epidemiology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Contemp Clin Trials Commun. 2022 Dec 23;31:101054. doi: 10.1016/j.conctc.2022.101054. eCollection 2023 Feb.
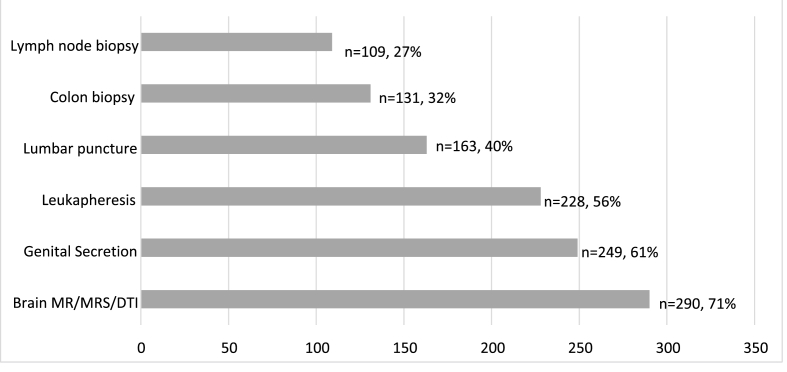
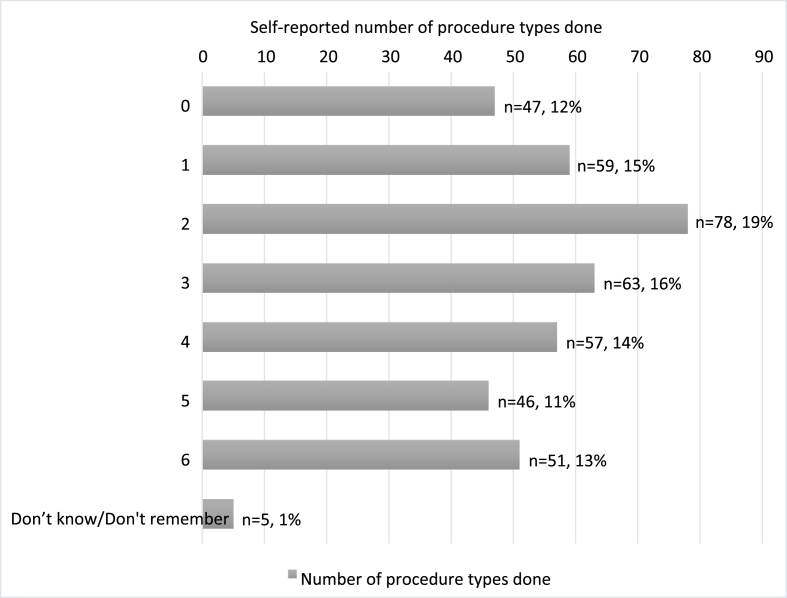
Clinical research regularly includes required, nontherapeutic procedures to answer research questions. Optional procedures usually offer minimal or no personal benefit and may involve harms and burdens. Members from the Bangkok SEARCH010/RV254 HIV research cohort of individuals acutely HIV-infected are recruited to six optional procedures varying in invasiveness: leukapheresis, genital secretions collection, lumbar puncture, brain MRI/MRS/DTI, colon biopsy, and lymph node biopsy. We surveyed cohort members about their first recruitment for each procedure to examine factors associated with decision making and attitudes about compensation. 406 members (68%) completed the survey. Reported procedure participation ranged from 71% (MRI) to 27% (lymph node biopsy). Respondents underwent 0-6 procedure types (median 3). Ordinal regression indicated that lower perceived HIV impact and HIV remission trial participation were associated with more procedures completed. Reports of decision difficulty varied, and feeling pressured by research staff was low overall. Notably, those who declined procedures and those who underwent more invasive procedures reported greater decision difficulty and perceived pressure. Most respondents felt compensation amounts were appropriate, although opinions differed by procedure, and for some procedures, between people who agreed and declined. There is limited literature regarding consent to and attitudes about optional research procedures. Researchers must consider how to best support voluntary decisions for procedures with little personal benefit, particularly in lower-income or marginalized populations. In this longitudinal research cohort, perceived pressure to participate may be a concern, although our finding of variation in participation rates corresponding to invasiveness is reassuring. Data from different research contexts would provide important comparators.
临床研究通常包括为回答研究问题而进行的必要的非治疗性程序。可选程序通常带来的个人益处极小或没有益处,且可能涉及危害和负担。招募曼谷SEARCH010/RV254急性HIV感染个体的HIV研究队列中的成员参与六种侵入性不同的可选程序:白细胞分离术、生殖器分泌物采集、腰椎穿刺、脑部MRI/MRS/DTI、结肠活检和淋巴结活检。我们就每位成员首次参与每种程序的情况进行了调查,以研究与决策以及对补偿的态度相关的因素。406名成员(68%)完成了调查。报告的程序参与率从71%(MRI)到27%(淋巴结活检)不等。受访者接受的程序类型为0至6种(中位数为3种)。有序回归表明,较低的感知HIV影响和参与HIV缓解试验与完成更多程序相关。关于决策困难的报告各不相同,总体而言,研究人员带来的压力较小。值得注意的是,拒绝程序的人和接受侵入性更强程序的人报告的决策困难和感知压力更大。大多数受访者认为补偿金额是合适的,不过不同程序的看法存在差异,对于某些程序,同意和拒绝的人之间也存在差异。关于可选研究程序的同意和态度的文献有限。研究人员必须考虑如何最好地支持对个人益处不大的程序做出自愿决策,尤其是在低收入或边缘化人群中。在这个纵向研究队列中,参与的感知压力可能是一个问题,不过我们发现参与率随侵入性而变化这一结果令人安心。来自不同研究背景的数据将提供重要的比较依据。